1/
This is a two part story (#RLR)
Each stands alone but their combination is multiplicative #Synergy #Interdependence
Today’s topic: “The sample is hemolyzed” - In vitro vs In vivo
This is a two part story (#RLR)
Each stands alone but their combination is multiplicative #Synergy #Interdependence
Today’s topic: “The sample is hemolyzed” - In vitro vs In vivo
2/
The lab notifies you “the sample is hemolyzed.”
First step in reasoning, did the hemolysis occur in the patient (in vivo) or during collection of the specimen (in vitro “ex vivo”), eg., prolonged application of tourniquet
The lab notifies you “the sample is hemolyzed.”
First step in reasoning, did the hemolysis occur in the patient (in vivo) or during collection of the specimen (in vitro “ex vivo”), eg., prolonged application of tourniquet
3/
In vivo hemolysis -> need to determine cause of hemolysis
In vitro hemolysis -> usually consequence of collection technique
In vivo hemolysis -> need to determine cause of hemolysis
In vitro hemolysis -> usually consequence of collection technique
4/
The NO MISS scenario is that the hemolysis is happening in the patient and it's your job to stop it!
The NO MISS scenario is that the hemolysis is happening in the patient and it's your job to stop it!
5/
The first step?
Study the scene of the crime - the peripheral smear.
Schistocytes → Microangiopathic hemolytic anemia
Spherocytes → Autoimmune hemolytic anemia/Hereditary spherocytosis
The first step?
Study the scene of the crime - the peripheral smear.
Schistocytes → Microangiopathic hemolytic anemia
Spherocytes → Autoimmune hemolytic anemia/Hereditary spherocytosis
6/
Believe it or NOT, you might also see bugs in your RBCs.
Yes - BUGS!
Malaria and Babesia are the biggest culprits.
Believe it or NOT, you might also see bugs in your RBCs.
Yes - BUGS!
Malaria and Babesia are the biggest culprits.
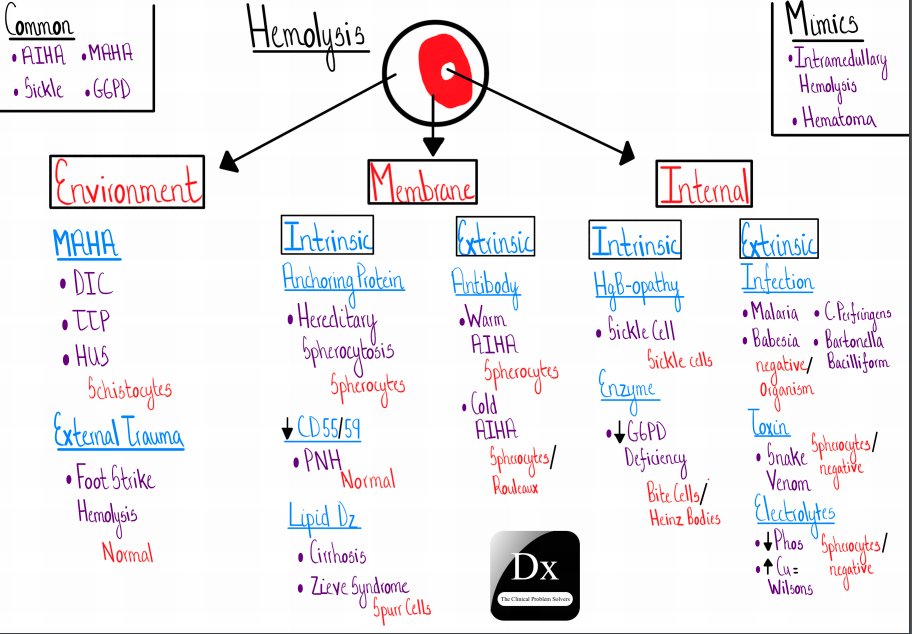
7/The smear is a great place to start, but let’s get systematic for a hot sec.
To approach hemolysis, the primary issue may be:
1. The environment - e..g, MAHA
2. The membrane -e.g, AIHA
3. Inside the cells - e.g, the BUGS!
A video walk through here:bit.ly/3cuyT9T
To approach hemolysis, the primary issue may be:
1. The environment - e..g, MAHA
2. The membrane -e.g, AIHA
3. Inside the cells - e.g, the BUGS!
A video walk through here:bit.ly/3cuyT9T
8/
Conclusion:
1. The smear is crucial in the approach to hemolysis.
2. Systematically study whether hemolysis is a problem in the environment, the membrane or inside the cell.
Conclusion:
1. The smear is crucial in the approach to hemolysis.
2. Systematically study whether hemolysis is a problem in the environment, the membrane or inside the cell.