1/ Can hemolytic anemia exist with no reticulocytosis?
Incoming #MedTwitter #Tweetorial #HemOnc #heme #hematology
Incoming #MedTwitter #Tweetorial #HemOnc #heme #hematology
2/ We've all been taught that hemolysis and hemorrhage are accompanied by a compensatory marrow response which leads to reticulocytosis and a slight increase in MCV (reticulocytes are larger than your average RBC).
But what if hemolysis co-existed with reticulocytopenia?
But what if hemolysis co-existed with reticulocytopenia?
3/ A 46 y.o. M with no significant PMH and PSH presented after he noticed a change in his urine color (darker) for the past wk. He mentions that the last 2 times he tried to donate blood in the past year, he was told he was too anemic to donate. Prior to this, no issues donating.
4/ Using @rabihmgeha's approach:
- Foreground: change in urine color.
- Middleground: recent-onset anemia?
- Distant background: no known anemia.
What has been going on for the past year? Why has urine been darker this past week?
- Foreground: change in urine color.
- Middleground: recent-onset anemia?
- Distant background: no known anemia.
What has been going on for the past year? Why has urine been darker this past week?
5/ On physical exam, patient's vitals were normal. He had yellow sclerae. No other exam abnormalities noted.
Labs: BMP normal. T bili 2.2 (D 0.7), D-dimer 1.8, fibrinogen 225, PTT 25.2, INR 1.42, CK 40, WBC 1.2 (24.7% N, 65% L, 0% E), Hgb 3.9, Hct 11.3, Plt 26.
Labs: BMP normal. T bili 2.2 (D 0.7), D-dimer 1.8, fibrinogen 225, PTT 25.2, INR 1.42, CK 40, WBC 1.2 (24.7% N, 65% L, 0% E), Hgb 3.9, Hct 11.3, Plt 26.
6/ Patient seems to have pancytopenia with severe anemia. 🧐
More labs: MCV 107, haptoglobin<10, LDH> 2000, ferritin 506, TSAT 26%, reticulocytes 1.3%, RPI 0.14, peripheral smear with anisocytosis/some macrocytes/some elliptocytes.
More labs: MCV 107, haptoglobin<10, LDH> 2000, ferritin 506, TSAT 26%, reticulocytes 1.3%, RPI 0.14, peripheral smear with anisocytosis/some macrocytes/some elliptocytes.
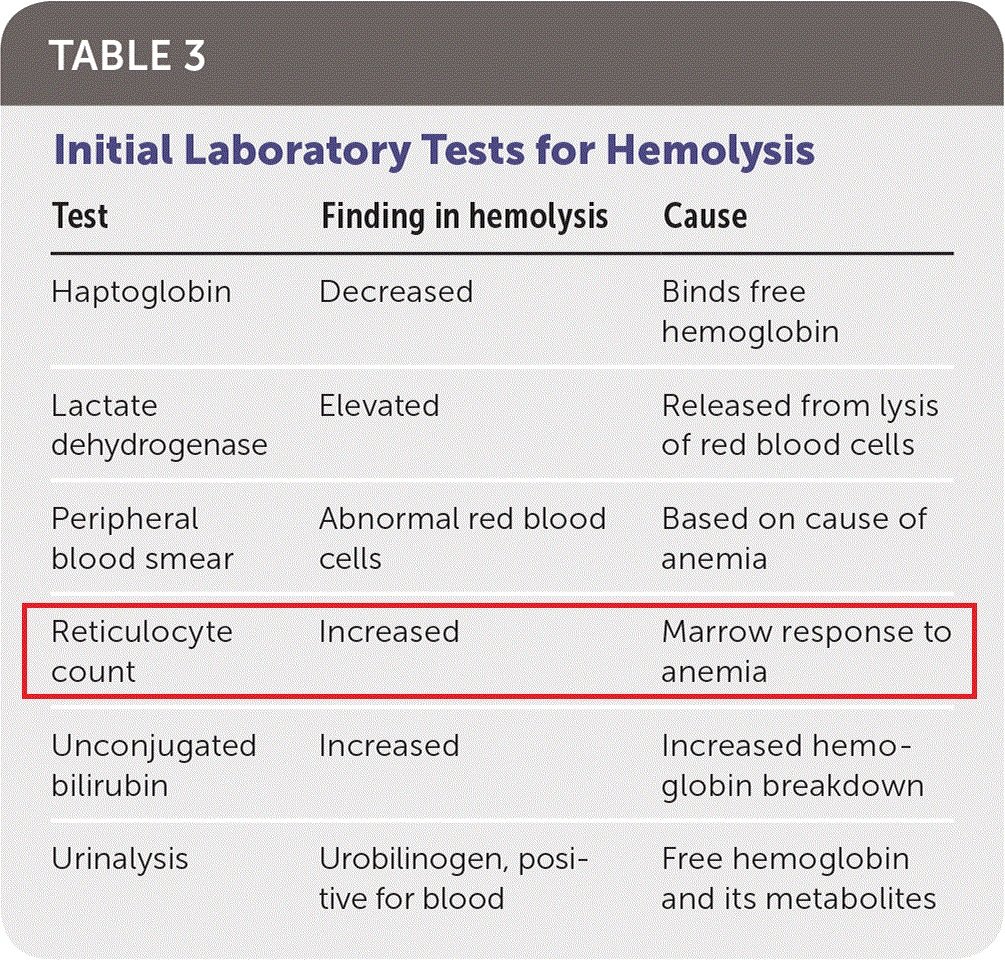
7/ How to interpret the reticulocyte indices?
Reticulocyte "count" is actually a % of the number of RBCs. In anemia, patient's RBCs are⬇️, creating an erroneously ⬆️reticulocyte count. We use the reticulocyte production index (RPI), or corrected reticulocyte count (CRC), instead.
Reticulocyte "count" is actually a % of the number of RBCs. In anemia, patient's RBCs are⬇️, creating an erroneously ⬆️reticulocyte count. We use the reticulocyte production index (RPI), or corrected reticulocyte count (CRC), instead.

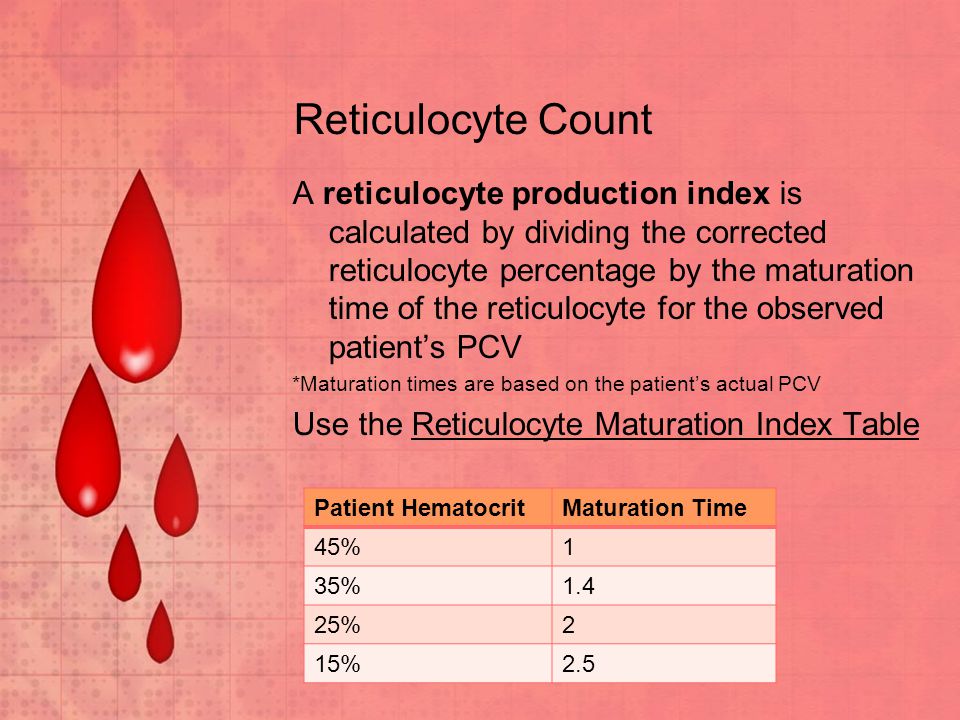
8/ The next step is to correct for the longer life span of prematurely released reticulocytes in the blood.
In this case: RPI = (1.3 x (11.3/42))/2.5 = 0.14
You can use MDCalc to help with the process: mdcalc.com/absolute-retic…
In this case: RPI = (1.3 x (11.3/42))/2.5 = 0.14
You can use MDCalc to help with the process: mdcalc.com/absolute-retic…
9/ If RPI <2, anemia is hypoproliferative. If RPI > 2, bone marrow is responding adequately.
10/ Our patient is presenting with hemolytic anemia, reticulocytopenia and pancytopenia.
Reticulocytosis (RPI>2) is a hallmark of hemolytic anemia (marrow responds to peripheral destruction of cells by⬆️reticulocyte production). Maybe pancytopenia holds the clue in this case?🤔
Reticulocytosis (RPI>2) is a hallmark of hemolytic anemia (marrow responds to peripheral destruction of cells by⬆️reticulocyte production). Maybe pancytopenia holds the clue in this case?🤔
11/ More labs:
Direct Coombs test: negative/HIV 1/2 Ab + p24 Ag: negative/Folate: 11 (N: 7-31)/Copper, Zn: normal levels/ADAMTS13 activity>79%/PNH flow cytometry: negative
Vitamin B12 level was <150. Methylmalonic acid level was 64 (N<0.4).
Direct Coombs test: negative/HIV 1/2 Ab + p24 Ag: negative/Folate: 11 (N: 7-31)/Copper, Zn: normal levels/ADAMTS13 activity>79%/PNH flow cytometry: negative
Vitamin B12 level was <150. Methylmalonic acid level was 64 (N<0.4).
12/ Well, patient has severe B12 deficiency, explaining his pancytopenia and macrocytic anemia. Upon further questioning, he mentioned having paresthesias in his feet for the past few months.
But does vitamin B12 deficiency explain the picture of hemolysis? Can't find it here⬇️
But does vitamin B12 deficiency explain the picture of hemolysis? Can't find it here⬇️

13/ Approximately 10% of patients with B12 deficiency experience life threatening hematological manifestations such as pancytopenia, pseudomicroangiopathy, severe anemia, or hemolysis. Rarely mentioned in hemolysis schemas, Vitamin B12 deficiency is the culprit in ~1.5% of cases.

14/ Reticulocytosis is a part of the hemolytic syndrome. Pernicious anemia is an exception. The bone marrrow in pernicious anemia may produce 4-5x the normal number of RBCs yet the reticulocyte count is low.
15/ The problem is impaired DNA synthesis/maturation, along with erythroblast apoptosis, resulting in anemia from ineffective erythropoiesis. Hemolysis, if present and significant, is intramedullary.
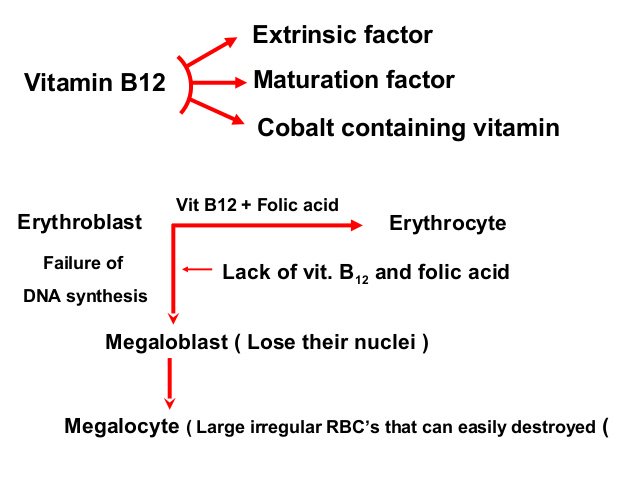
16/ Staining of marrow demonstrates ample reticulum substance in the cytoplasm of the nucleated erythroid cells. But the cytoplasm matures (causing megaloblastosis) and the reticulum substance (ribosomal RNA defining reticulocytes) disappears before the nucleus is lost. ❌retics
17/ Another instance of hemolysis with reticulocytopenia: aplastic crisis that may strike patients with chronic hemolytic anemias. Peripheral hemolysis persists while erythropoiesis siderated by parvovirus B19.
Rapidly developing anemia = reticulocytopenia in the initial stages.
Rapidly developing anemia = reticulocytopenia in the initial stages.
18/ Back to our patient:
Gastrin: 108 (N: 0-115)/Anti-IF antibody: 2.4 (N<1.1)/Anti-parietal cell antibody: 33.8 (N<20).
He was diagnosed with pernicious anemia. Had a family history of auto-immune diabetes.
Gastrin: 108 (N: 0-115)/Anti-IF antibody: 2.4 (N<1.1)/Anti-parietal cell antibody: 33.8 (N<20).
He was diagnosed with pernicious anemia. Had a family history of auto-immune diabetes.
19/ Treated with IM injections of vitamin B12. No bone marrow aspiration/biopsy were done given that B12 deficiency explained most of the abnormalities. Note the sharp reticulocytosis a few days later coupled with improvement in hemolysis markers and WBC/RBC/platelet counts.

20/ Re-evaluated in clinic one month later: Hgb 11.1 WBC 8.5 Platelet count 389 LDH 232 Haptoglobin 207 MCV 98.6. ✌️
Take-home points:
- While hemolysis is known to cause reticulocytosis (RPI>2), there are some exceptions: B12 deficiency (intramedullary maturation problem), chronic peripheral hemolysis with aplastic crisis, brisk hemolysis in the very early stages (bone marrow overwhelmed).
- While hemolysis is known to cause reticulocytosis (RPI>2), there are some exceptions: B12 deficiency (intramedullary maturation problem), chronic peripheral hemolysis with aplastic crisis, brisk hemolysis in the very early stages (bone marrow overwhelmed).
- B12 deficiency is a (rare) cause of hemolysis. Think of it when you have pancytopenia, megaloblastosis, malabsorption syndromes, history of gastric bypass, paresthesias or AMS.
- A BMB (invasive) can be potentially avoided if anomalies respond to aggressive B12 supplementation
- A BMB (invasive) can be potentially avoided if anomalies respond to aggressive B12 supplementation
Further reading:
- shmabstracts.com/abstract/vitam…
- longdom.org/open-access/he…
- PRUTHI, R. K., & TEFFERI, A. (1994). Pernicious Anemia Revisited. Mayo Clinic Proceedings, 69(2), 144–150.
- shmabstracts.com/abstract/vitam…
- longdom.org/open-access/he…
- PRUTHI, R. K., & TEFFERI, A. (1994). Pernicious Anemia Revisited. Mayo Clinic Proceedings, 69(2), 144–150.