The story is a little more complicated than “stay 6 feet away” guidelines. Coronavirus risk is simply not one-dimensional. We need to discuss high-risk activities & environments. I spoke w @B_resnick & discussed 4 dimensions of transmission risk #COVID19
vox.com/science-and-he…
vox.com/science-and-he…
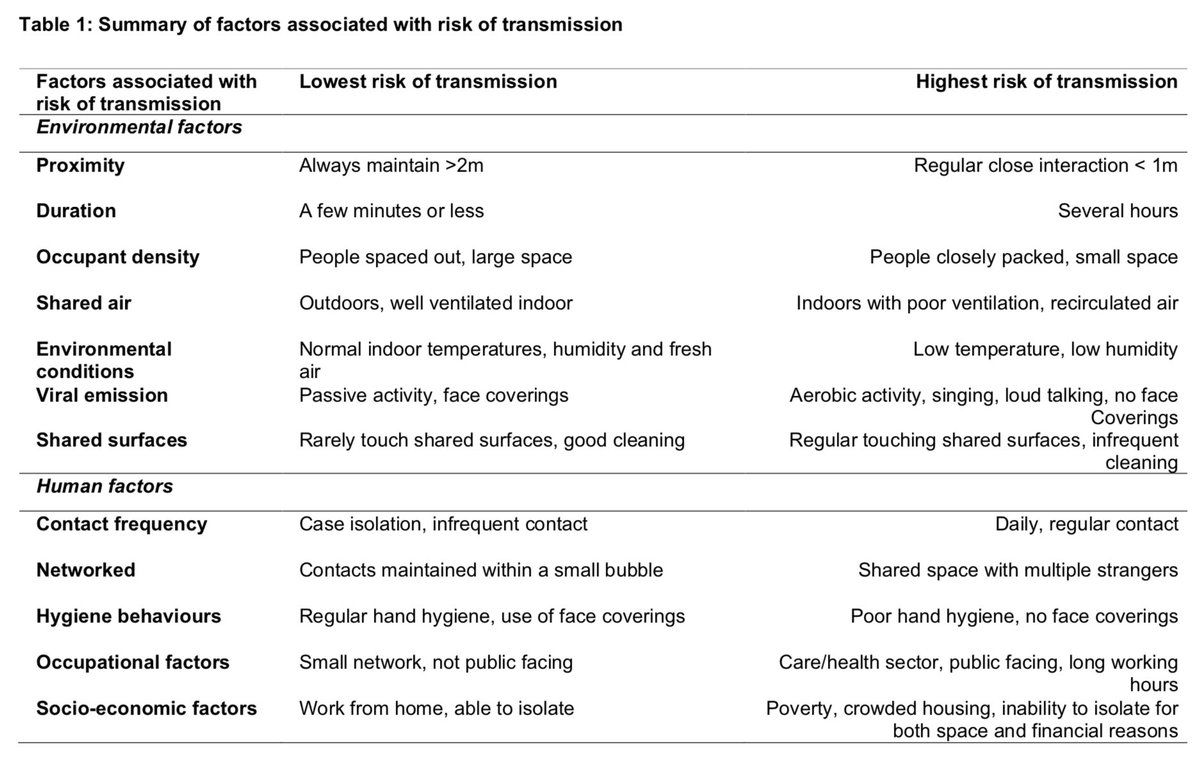
We need to think about risk in four dimensions: distance to other people, environment, activity, and time spent together.
A crowded indoor place, with poor ventilation, filled with people talking, shouting, or singing for hours on end will be the riskiest scenario. A sparsely populated indoor space with open windows is less risky (but not completely safe).
On the other end of the spectrum running quickly past another jogger outside is minimal risk. There are many scenarios in between. In general, outdoors is lower risk. But if you have a gathering outside, and you spent all day together with your friends, risk is still higher.
And it’s not just the location or the time spent together: The activity people are engaged in matters, too.
In Washington state, a person with the virus attended a choir practice, and more than half of the other singers subsequently got sick. This was labeled a “superspreading” event, as one infection led to 32 others. Why was this so risky?
The convergence of many risk factors: singing, the time spent together (the practice was 2.5 hours), and the interaction between the choir members in an enclosed space (not only did they all practice together, they also split up into smaller groups and shared cookies and tea).
That’s why we need to think of risk in terms of many dimensions: so we can each think critically and not fall back on rules that are too simplified.
• • •
Missing some Tweet in this thread? You can try to
force a refresh