🦠 There’s a lot we don’t yet understand about Omicron, including its impact on immunity and what it means for vaccines. New data will be emerging over the next few wks, which could be misinterpreted w/o context. What we might expect & how to interpret the emerging data? 🧵(1/n)
1- Genomic data:
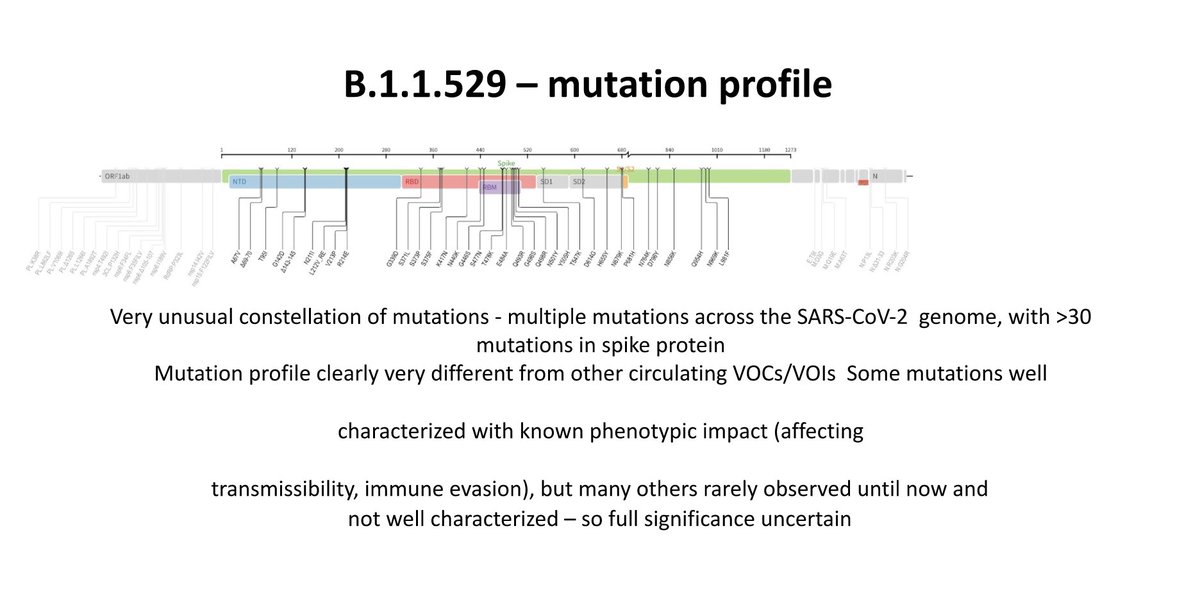
The biggest concern with omicron is that it contains >30 mutations in just the spike protein, the part which helps it enter human cells and the target for vaccines. This mutation profile is very different than other VOCs. (2/n)
The biggest concern with omicron is that it contains >30 mutations in just the spike protein, the part which helps it enter human cells and the target for vaccines. This mutation profile is very different than other VOCs. (2/n)

There are plausible biological consequences of some of these mutations, but we don't really know the combined effect of all these mutations, so full significance of omicron is uncertain.
https://twitter.com/jbloom_lab/status/1464005676842184705?s=20/(3/n)
For how long Omicron has been circulating is an important question. Most estimates land ~mid October & identification of cases with no travel links to SSA indicates early evidence of community transmission. See threads by @K_G_Andersen & @trvrb
https://twitter.com/K_G_Andersen/status/1465824067101986820?s=20(4/n)

2- Epidemiological data:
Epi data could give clues re the growth rate. There are several analyses about Gauteng indicating omicron seems to spread quickly, Rt increasing from ~0.8 to >2. Prelim evidence from SA suggests this might be driven by increased risk of reinfection.(5/n)
Epi data could give clues re the growth rate. There are several analyses about Gauteng indicating omicron seems to spread quickly, Rt increasing from ~0.8 to >2. Prelim evidence from SA suggests this might be driven by increased risk of reinfection.(5/n)

It’s especially concerning that omicron is increasing not only in Gauteng province but also in other parts of South Africa, which could be an indication that the rapid rise is likely not due to other factors such as behaviour. (6/n)


So, putting all these observations together, we can make an assumption that there might be a correlation between omicron and increased rates of infection. But how can we know whether the increasing frequency reflects the fitness advantage or chance? (7/n)
3- Modelling data
Rapid displacement of existing Delta by Omicron in SA is a key clue that it’s likely growing fast, at least in a pop w/ 25% vax rate & high immunity from prior infection. We don’t really know whether similar picture will play out in other countries (8/n)
Rapid displacement of existing Delta by Omicron in SA is a key clue that it’s likely growing fast, at least in a pop w/ 25% vax rate & high immunity from prior infection. We don’t really know whether similar picture will play out in other countries (8/n)

We've seen other variants that had us concerned — beta, would be the best example. While it had an impact on immune response, it’s been outcompeted w/ intrinsically more transmissible variant, delta. We don't know the answer as to how this is going to go for omicron. (9/n)
One of the strongest pieces of evidence to monitor is the trend in other countries, not only increase in omicron cases as this is expected, but the replacement of delta. For instance, incidental S-gene target failure (SGTF) seems to be a proxy for omicron due to 69-70del. (10/n)
Data from England shows a recent uptick in cases w/ SGTF, but this is early data and could indicate importations & linked secondary cases rather than community transmission. So, researchers are carefully watching this data. Explainer by @_nickdavies
https://twitter.com/_nickdavies/status/1466204363110633476?s=20(11/n)

4- Immune response
Mutations in the omicron might mean the immune response generated by vaccination (or prior infection) may not target it as well. Important to remember that immune response provides multilayer protection – it is unlikely that all protection will be lost. (12/n)
Mutations in the omicron might mean the immune response generated by vaccination (or prior infection) may not target it as well. Important to remember that immune response provides multilayer protection – it is unlikely that all protection will be lost. (12/n)

When considering vaccine effectiveness against new variants, there are at least three elements to consider: doi.org/10.1016/j.cell… (13/n)

The primary way of measuring antibody (Ab) effectiveness in the lab is the neutralisation test. Neutralisation studies can tell us whether levels of Ab in the blood (convalescent and vaccinated plasma) are high enough to prevent the virus from infecting cells in the lab. (14/n)
In this test, we grow/culture the virus in the presence of antibodies. If the Ab is effective, we won’t see any growth b/c the virus has been ‘neutralised’. If the Ab is not effective, then we will see growth. But, it’s not a yes/no answer, there will be a range of growth.(15/n)

While neutralisation antibodies (NAb) are a correlate of protection, we don’t yet know the threshold they need to drop below b4 they completely loose efficacy. And vaxxed individuals already have a very high NAbs to start with, which is orders of magnitude above IC90. (16/n)
Also neutralisation assays are challenging to run & difficult to optimise. Prev studies indicate that nAb assays are very sensitive - 10 fold reduction in nAb doesn’t mean a 10x drop in clinical efficacy. So they need careful interpretation. nature.com/articles/s4154… (17/n)

Based on genomic data, we'll likely see a big drop in neutralisation activity (likely more decline with natural immunity than with vaccines) in these studies. But decreased neutralising activity in vitro does not on its own predict that vaccines will be ineffective. (18/n)
.@PaulBieniasz et al. looked at the impact of a polymutant spike w/ 20+ mutations & showed a significant reduction of neutralisation in pseudovirus neut assays. But, plasma from infected + vaxxed ppl retained significant neutralisation activity nature.com/articles/s4158… (19/n)
Despite a significant decline in NAb response, all vaccinated individuals retained neutralization vs Delta w/ 2 doses. In clinical studies, vaccine effectiveness was not affected against disease and modestly declined against infection. (20/n)
https://twitter.com/mugecevik/status/1430218372348878860?s=20
Again, despite a very big drop in neutralisation response against Beta variant, all vaccinated individuals retained neutralisation capability. And contrary to many peoples' claim that vaccines don’t work against beta, almost all vaccines retained some effectiveness. (21/n)

If we look at the relative protection against other variants, T cell responses have wide repertoire across spike with individual variation by HLA. So, T cell responses are generally far more robust and are less impacted by mutations than the neutralising antibody response. (22/n)

Memory B & T cells remain in blood, which will rapidly boost NAb levels after subsequent infection w/ the actual virus. So whilst the ability of a persons sera to neutralise the virus is desirable, it is certainly not essential when it comes to protecting against disease. (23/n)
In summary: these data suggest that Omicron seems to be growing fast, either due to intrinsic transmissibility and/or immune erosion, but we don't know if & how much w/absolute certainty.
https://twitter.com/trvrb/status/1466076761427304453?s=20(24/n)

The main concern is the immune erosion potential. While NAb studies will likely give worrying results, once we start to get some real-world studies into how things are doing, my guess is that vaccines will still be doing a decent job in protecting ppl from getting sick. (25/n)
If there is a drop in neutralisation, we would expect more vaccinated people to suffer infections. However, this reduction may well be far less pronounced when it comes to moderate/severe disease and death as the other aspects of the defences are less impacted by variants. (26/n)
In the meantime, most importantly the focus should be on reinforcing efforts to deliver primary doses of vaccines globally, as these countries will be affected the most, as already countries with low vaccination rate are fairing worst. (27/n)

And there are several options that could improve vaccination strategies. In addition to the below list, booster doses are shown to boost the NAb levels, which could give us a head start before the omicron wave. by @apsmunro et al. thelancet.com/journals/lance… (28/n)

So, we’re not expected to go back to “square one”. And beware of ppl 🚨 suggesting vaccines no longer work vs omicron based on early lab data. By far the most important evidence to look out for is vaccine effectiveness based on clinical data theatlantic.com/science/archiv… (29/n)
There are many unknowns. We don't know if it will influence the severity of illness, reinfection, effectiveness of vaccines and treatments. So, there’s still a lot of work to be done, including lab experiments, contact tracing studies.@heidiledford nature.com/articles/d4158… (30/n)
For example, if omicron doesn’t have intrinsic transmissibility advantage over delta but has partial immune escape, whether it will be able to outcompete other variants and cause significant disease burden. Great paper by @BillHanage @mlipsitch cell.com/cell/fulltext/… (31/n)

There are some preliminary reports indicating omicron cases may be mild. While this is better than hearing worst outcomes, it is too early to conclude one way or another, as it is challenging to analyse severity as we discussed w/ @sharmista here thelancet.com/journals/lanin… (32/n)
We’ve got to be really careful especially as scientists and doctors because there’s already a lot of speculation and misinformation about this particular variant and getting answers may take a few weeks or months. I will update this thread as more data becomes available (33/n)
Don’t forget immune responses are not all or nothing. Antibodies are important, but the immune response is so much more than that. The immune system is complex but very cool. Visual by @SaundersNell1 titled "Infection", depicting the immune response to #SARSCoV2 infection. (34/n)

Finally, science says borders don't stop viruses. If omicron is more transmissible, it will be identified everywhere. The biggest problem is vaccine inequity. Even if we boost all our populations in HICs, we might face another variant if 60% of the world remains unvaxxed. (35/n)
This thread is partially based on our paper in the @CellPressNews . Many thanks to my co-authors @NathanGrubaugh @VirusesImmunity @p_openshaw Link to the paper: doi.org/10.1016/j.cell… (36/n)

Preliminary neutralisation studies indicate that 2 doses of vaccines may not be sufficient to prevent *infection* w/ omicron (not severe disease), but regular boosters will help restore this decline to an extent. Clinical effectiveness studies to follow.
https://twitter.com/mugecevik/status/1468339178421342212?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh