Webinar is now LIVE. I’ll be providing some coverage on Twitter.
@DrMCecconi is describing his experience.
It’s been written up here jamanetwork.com/journals/jama/…
And he did a superb webinar with @JAMA_current where he spoke directly from the front lines esicm.org/blog/?p=2626
It’s been written up here jamanetwork.com/journals/jama/…
And he did a superb webinar with @JAMA_current where he spoke directly from the front lines esicm.org/blog/?p=2626

They used an ICM network already in place for ECMO referrals to communicate and share resources
They closed elective surgery and created surge ICU capacity ASAP
And then made sure their message was spread out to the world - GET READY
esicm.org/covid-19-updat…
They closed elective surgery and created surge ICU capacity ASAP
And then made sure their message was spread out to the world - GET READY
esicm.org/covid-19-updat…
On the 17th of March (their peak) 151 patients were admitted to ICU in Lombardy
To put that in perspective that’s 20% of their pre-surge ICU capacity
Average LOS 10-14 days jamanetwork.com/journals/jama/…
To put that in perspective that’s 20% of their pre-surge ICU capacity
Average LOS 10-14 days jamanetwork.com/journals/jama/…
How they created their surge capacity has also been documented
Separating of patients into COVID and non-COVID streams was key
onlinelibrary.wiley.com/doi/abs/10.111…
Separating of patients into COVID and non-COVID streams was key
onlinelibrary.wiley.com/doi/abs/10.111…
Simulation was so important- donning, doffing, proning etc
advancesinsimulation.biomedcentral.com/articles/10.11…
advancesinsimulation.biomedcentral.com/articles/10.11…
@ESICM created guidelines for surge capacity esicm.org/wp-content/upl…
@DrMCecconi et al were amongst the first to notice the increased risk of thrombosis ncbi.nlm.nih.gov/m/pubmed/32367…
They’ve just had a recent paper accepted on their learning points from COVID19 (check @yourICM for its publication)
In the meantime here’s a personal perspective from @avkwong healthmanagement.org/c/icu/issueart…
In the meantime here’s a personal perspective from @avkwong healthmanagement.org/c/icu/issueart…

Prone positioning found to be very helpful
Inhaled NO not so
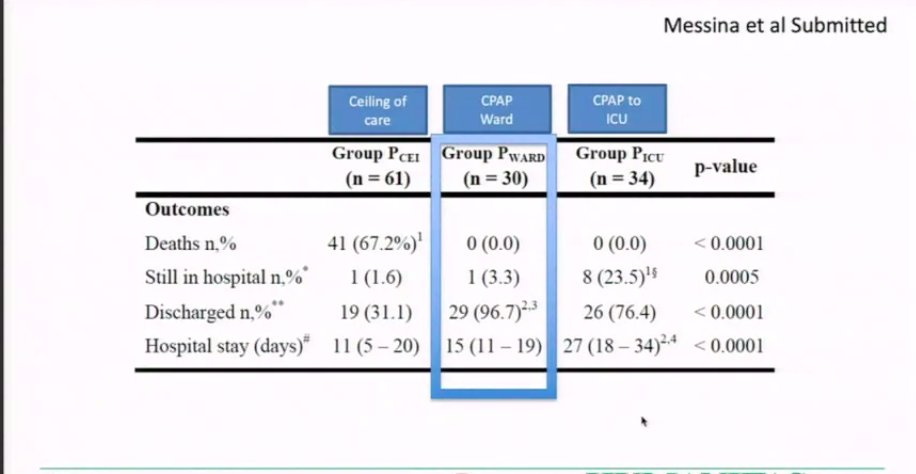
Their experiences with CPAP were interesting. A need for PS on top of CPAP was strong predictor of intubation
Inhaled NO not so
Their experiences with CPAP were interesting. A need for PS on top of CPAP was strong predictor of intubation
Some of their data on CPAP use and outcomes
@DrMCecconi describes not changing his practice regarding selection of respiratory support for patients. Many of us have reached similar conclusions.
@DrMCecconi describes not changing his practice regarding selection of respiratory support for patients. Many of us have reached similar conclusions.
He describes the experience as “tiring, yet fulfilling”
And warns us to “not be surprised twice”.
-increase ICU competencies
-have a “mobile ICU army”
-work in networks
-protect patients and staff
-do research
-continue to contain the disease in community and in hospitals
And warns us to “not be surprised twice”.
-increase ICU competencies
-have a “mobile ICU army”
-work in networks
-protect patients and staff
-do research
-continue to contain the disease in community and in hospitals
Now @JKesecioglu discussing ethics
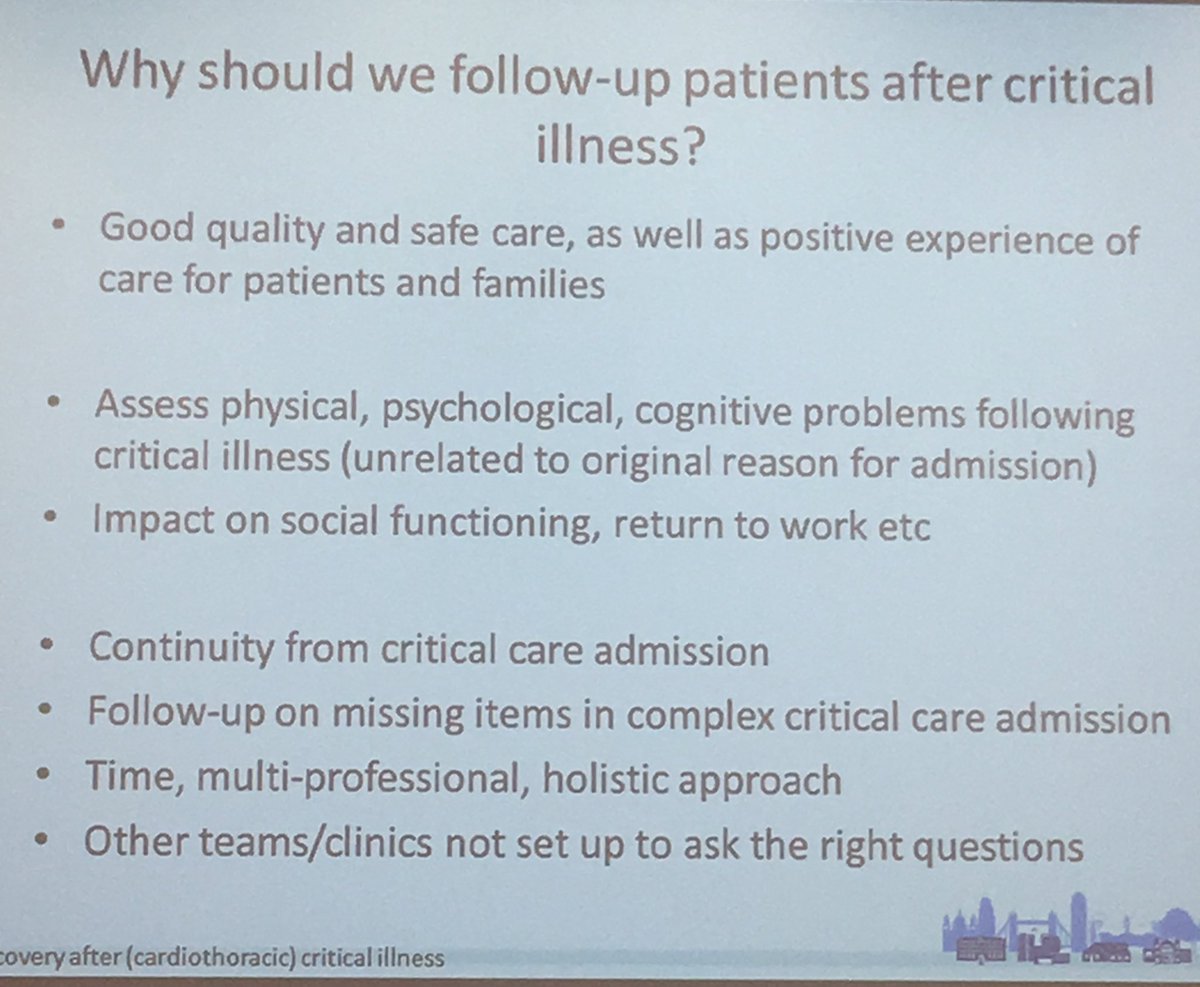
Over time ICU has moved from focusing on survival to looking at wellbeing of both patients and staff
Especially as we recognised that what we do on the unit has long term effects ncbi.nlm.nih.gov/pmc/articles/P…
Over time ICU has moved from focusing on survival to looking at wellbeing of both patients and staff
Especially as we recognised that what we do on the unit has long term effects ncbi.nlm.nih.gov/pmc/articles/P…
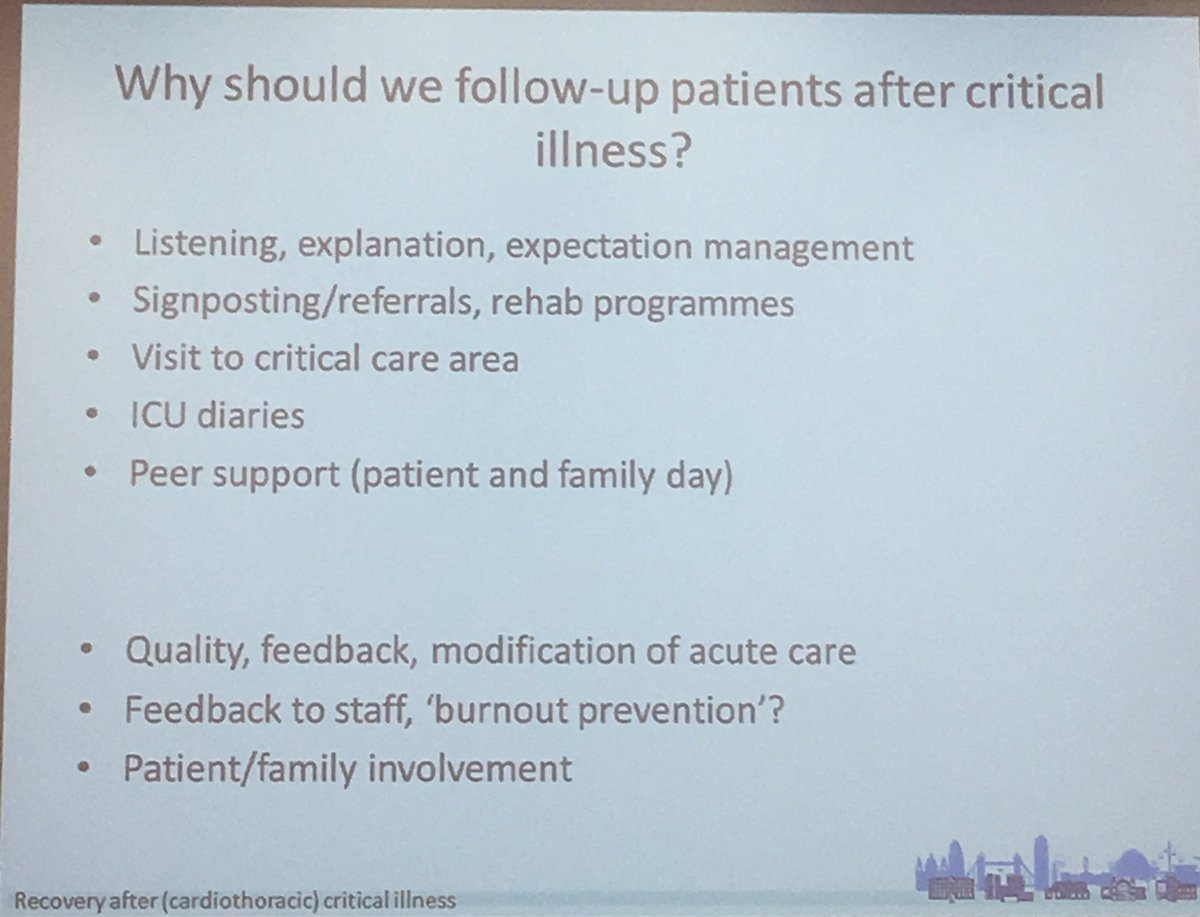
Humanising the intensive care unit is critically important
Follow @HUMANIZALAUCI for more on this
journals.lww.com/ccmjournal/ful…
Follow @HUMANIZALAUCI for more on this
journals.lww.com/ccmjournal/ful…
Things like open visiting, nice decorations, and continual compassionate communication go a long way towards improving the experience of the ICU patient.
Sadly during #COVID19 a mix of surge capacity and the risk of cross infection made this very difficult.
Sadly during #COVID19 a mix of surge capacity and the risk of cross infection made this very difficult.
PPE distanced the bedside carer’s from the patients.
Isolation distanced the patients from their families.
Delirium has been commonplace.
Isolation distanced the patients from their families.
Delirium has been commonplace.
It’s worth remembering that ARDS doesn’t just affect the short term.
Some patients still have issues with physical function up to 5 years after
pubmed.ncbi.nlm.nih.gov/21470008/
Some patients still have issues with physical function up to 5 years after
pubmed.ncbi.nlm.nih.gov/21470008/
Families also experience significant PTSD ncbi.nlm.nih.gov/pmc/articles/P…
What about healthcare providers?
We faced a new situation, making challenging decisions under extreme pressures
We were also worried about our health and those of our families/friends...
We faced a new situation, making challenging decisions under extreme pressures
We were also worried about our health and those of our families/friends...
This led to significant moral injury
(I am still living with some effects of this).
Studies are coming out demonstrating the mental toll of acute care in #COVID19 potloc.com/blog/en/potloc…
(I am still living with some effects of this).
Studies are coming out demonstrating the mental toll of acute care in #COVID19 potloc.com/blog/en/potloc…
Recent @bmj_latest article describes this too bmj.com/content/368/bm…
Be honest with staff about what’s going to happen.
Support them- psychologists on tap is very helpful.
Compassionate leadership helps.
Some great resources are available thanks to @DrJulie_H ics.ac.uk/ICS/Education/…
Support them- psychologists on tap is very helpful.
Compassionate leadership helps.
Some great resources are available thanks to @DrJulie_H ics.ac.uk/ICS/Education/…
After the peak, don’t forget to look after staff still.
Debrief.
Prepare for a potential second peak.
Debrief.
Prepare for a potential second peak.
Methods to prevent moral distress:
-enhanced decision making (make difficult decisions as a team rather than as individuals)
-give time and space for clinicians to decompress
-try and keep consistent teams to create mutual support
-enhanced decision making (make difficult decisions as a team rather than as individuals)
-give time and space for clinicians to decompress
-try and keep consistent teams to create mutual support
Looks like that’s a wrap folks
Till next time!
Till next time!