1/ Covid (@UCSF) Chronicles, Day 86
Grand Rounds today; here: bit.ly/2AiPTmj
First, George Rutherford update on Epi & @WHO fiasco. Then all-star panel discussion re: the tension between going fast & getting it right in Covid, w/ @califf001, @VPrasadMDMPH & @RFRedberg
Grand Rounds today; here: bit.ly/2AiPTmj
First, George Rutherford update on Epi & @WHO fiasco. Then all-star panel discussion re: the tension between going fast & getting it right in Covid, w/ @califf001, @VPrasadMDMPH & @RFRedberg
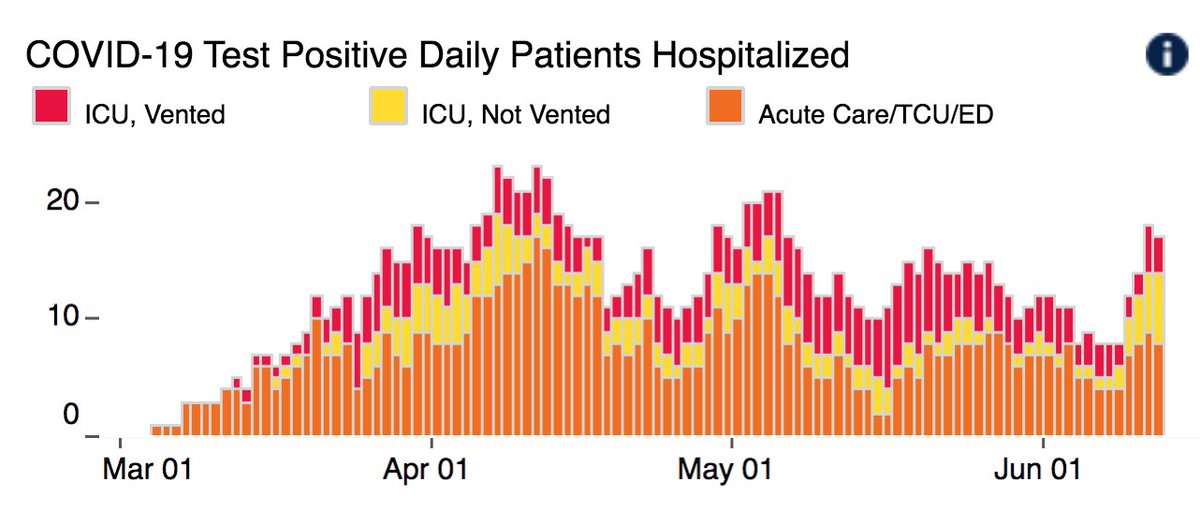
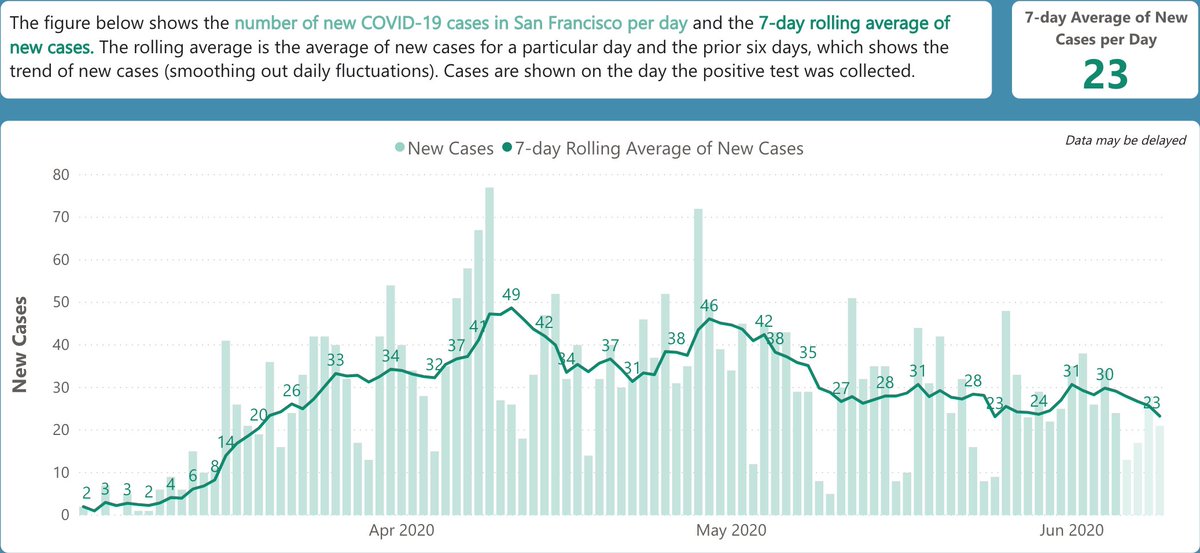
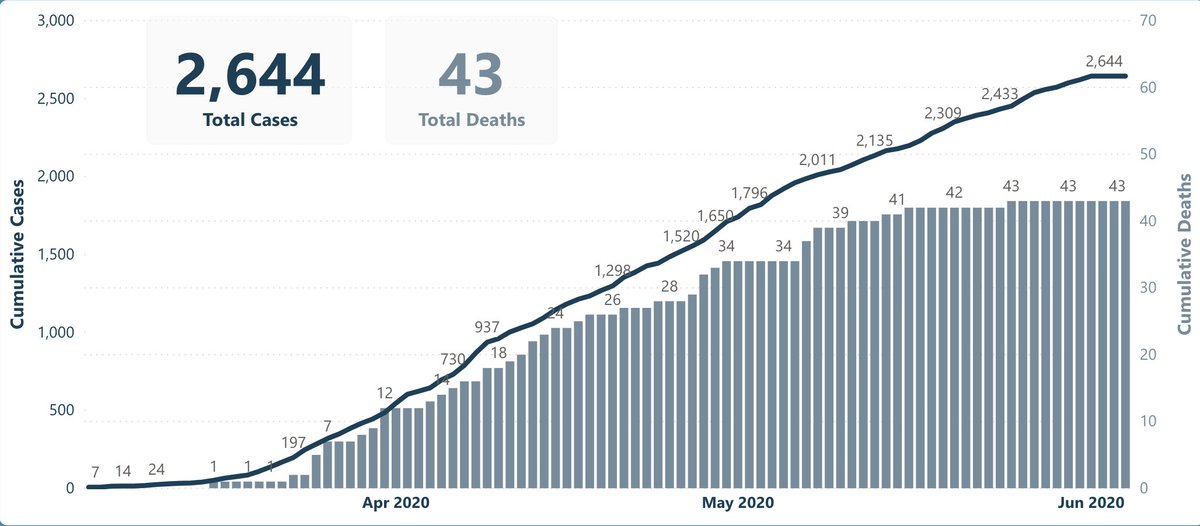
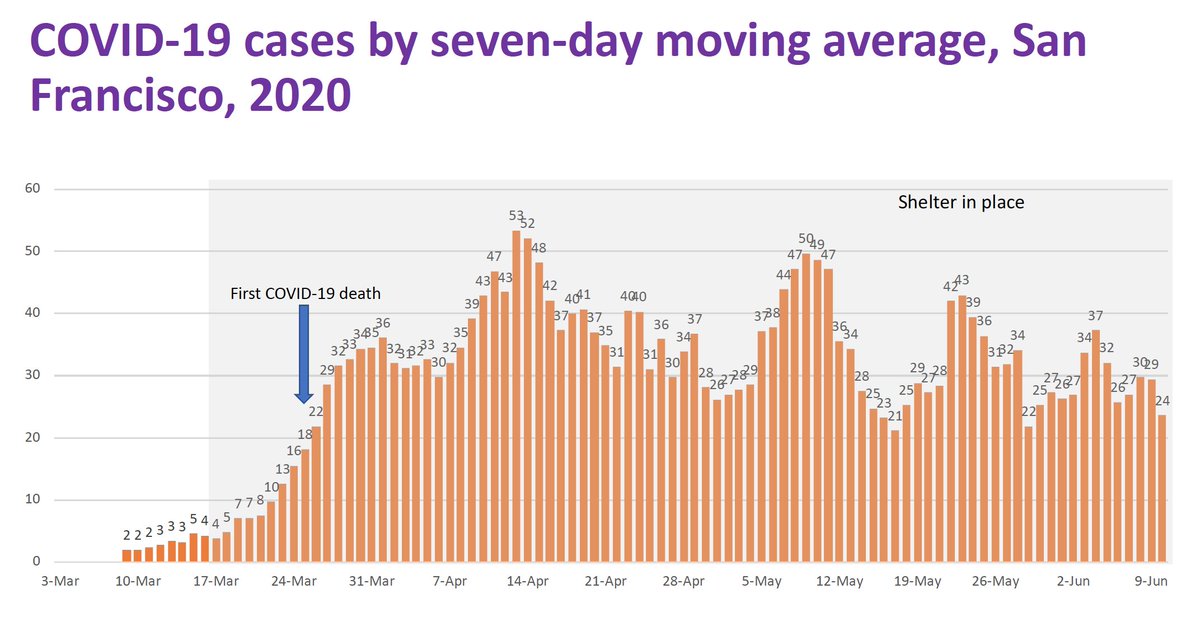
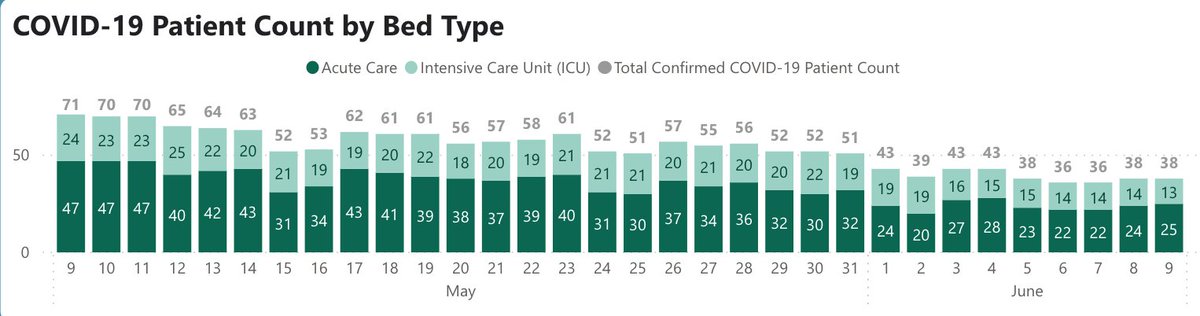
2/ First, local update. @UCSFHospitals, up to 16 pts, double 3d ago. Concerning. But overall SF cases (Fig L) and hospitalizations (Fig R) are stable, so @UCSF uptick is most likely a blip. Definitely bears watching.
George R. discusses SF, CA situation @ 10:40 on video.
George R. discusses SF, CA situation @ 10:40 on video.
3/ Note that the talk about a “surge in California” is sorta right (@ 8:35) - cases going up, but mostly in SoCal. Northern CA remains OK, though variation here too, with SF stable, mild upticks in Marin, Alameda. As George often says, North & South are two different epidemics.
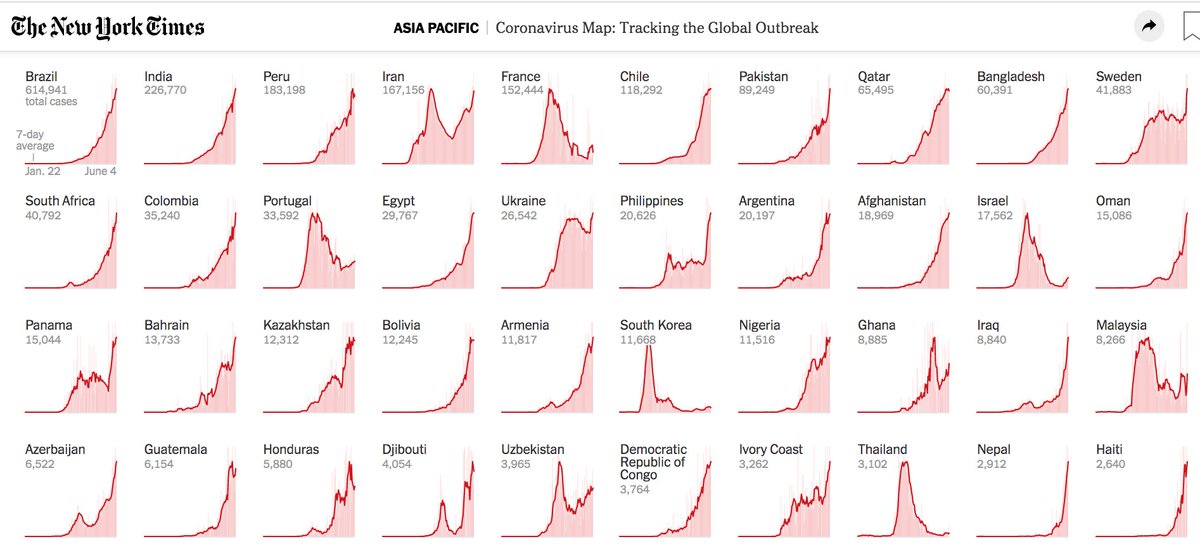
4/ @ 5:50: Rutherford: 418K deaths, 7M cases in world. US: ~2 million cases, 110K deaths. U.S. cases slowly falling, but rising in southeast & few midwest states. California averaging ~60 deaths/day, ~half of our expected share (based on population) of 1000 U.S. deaths/day.

5/ @ 7:15: No sign of spike in Minnesota or Washington DC (Fig) – we’re at about time when we might see cases from the protests, so reassuring. George: “They were outside, which is good; many people had masks on, which is good; tear gas is bad; shouting is bad. It’s a balance.”

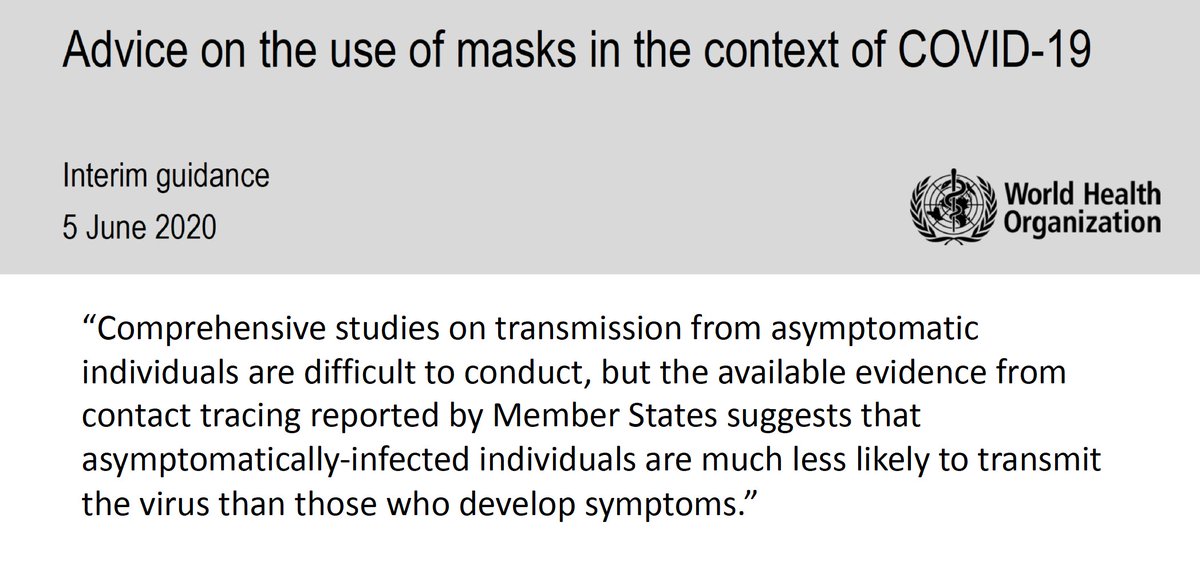
6/ @ 13:20: On Monday, @WHO put out statement below. George reviews evidence on asymptomatic spread: clear that it’s NOT rare. @ 14:50: “The trap that WHO stepped into” is confusing asymptomatic vs. pre-symptomatic transmission; former is uncommon, latter is not.
7/ @ 16:05: Q) Do asymptomatic/pre-symptomatic patients have lower viral loads than symptomatic pts? Answer: not really (study below). “We have to assume that people who are pre-symptomatic, & some who are asymptomatic… have similar viral loads to people who are symptomatic.”

8/ @ 18:45: Asymptomatic pts are capable of spread but less infectious since not coughing or sneezing. Best estimate: 1/2 as likely to spread as pts w/ symptoms. George: “Asymptomatic & pre-symptomatic infection are very real, very common, & the solution is to wear your mask.”

9/ @ 23:00: Q&A with George: Q) Is the virus getting milder. A) "No. There’s no evidence of that… The virus doesn’t watch TV. It doesn’t read the paper…. It has one purpose in life, & that’s to reproduce in YOU.”
10/ @ 23:40: Q: What explains variation in state-by-state cases? Some opened & doing OK, others have done everything right & gotten hit. A) Some element of luck, random variation. But ultimately, chances of surge are higher if states (and people) ignore public health recs.
11/ @ 26:20: Q) Does the outbreak in an Israeli school on.wsj.com/2UDd9lE alter general premise that kids are safer & transmit less? A) Israeli outbreak was in a high school, may be riskier at that age; no known outbreak in elementary schools, but evidence isn’t very robust.
12/ @ 28:00: Q) Are political rallies bad? A) Yes! Small group➔small chance of encountering Covid+ pt. But “if you go to a place with a zillion people," good chance of encountering Covid+ people. Trump will make folks sign a liability release for rallies bit.ly/2Yudp7B
13/ @ 29:30: Shift to chat w/ Califf, Prasad, Redberg (& George) re: tension between speed in pub/approval process, & risk of error. Rita: pre-Covid, 250 submits/mth @JAMAInternalMed; now 900. “And every submission comes w/ request to have it reviewed yest. & published last wk.”

14/ @ 33:00: Redberg: preprints “can be helpful.” But “they should have a big watermark: ‘Not for Clinical Use, Certainly Not for Therapies.’” Data: only 20% of preprints end up getting published in peer-reviewed journals. But many patients look at them & want to follow recs.
15/ @ 35:00: Prasad lists several errors that made it to literature: 1st @NEJM remdesivir study; alopecia as risk factor for Covid, others… all w/ classic statistical errors. “Is rate of errors different w/ Covid or is it just the compressed time-span?” he asks. A) Not clear yet
16/ @ 37:00: Vinay re: huge flak (eg, bayareane.ws/2x4UBlZ) over @stanford - Santa Clara antibody study. He believes reaction was polarized partly because authors had penned prior pieces re: lockdowns being overkill – thinks some of study critiques were legit, others too harsh
17/ @ 39:00: All FDA commissioners need to manage tension between speed & safety. When Rob Califf became commissioner, there was some consensus that – for otherwise untreatable diseases – best to tilt toward speed/approval, letting pts/families make choice whether to accept risk.
18/ @ 42:20: Califf enthusiastic re: using real-world data to assess drugs, “but no substitute for good methods.” Thinks FDA isn’t main problem; instead, healthcare delivery orgs don't enroll enough pts in trials; several reasons (time pressure, incentives, admitting uncertainty)
19/ @ 56:20: Redberg counters: Problem is FDA doesn’t require randomized data for drugs/devices, often approves based on observational data, surrogate endpoints. Califf: not just FDA problem; “Simply saying that FDA should do this… isn’t confronting the demon in your own house.”
20/ @ 59:30: Re: Surgisphere fiasco bit.ly/2BZlkm1. Prasad: peer-review is built on a foundation that submissions are truthful – it’s not very good at identifying fraud. But plenty of flashing red lights here, with a company no one had heard of having a massive data set.
21/ @ 1:02:20: Califf: hard to require 1st author to review every analysis, but must ask hard ?s re: data provenance. He believes 1st authors often haven’t written the paper. Wants to use #AI to check papers against authors' past writings; suspects we’d find tons of ghostwriting.
22/ @ 1:07:30, probably most fascinating segment: what happens if, in October, FDA is asked to approve a vaccine with borderline results. Califf: with the stakes so high, the FDA commissioner – who normally stays out of drug approval decisions – would have to get involved.
23/ Even scarier, Califf notes that Trump has the legal authority to make the decision; a nightmare scenario discussed by @ZekeEmanuel & @DrPaulOffit @nytimes nyti.ms/2AvzJWH. If vaccine is scientific slam dunk, this’ll be easy; but need to prepare for gray-zone results.
24/ Everyone, inc. Califf, agreed that gray-zone vaccine scenario is more likely than not. And want more? @ 1:12:00, what if it’s vaccine made in China? Mind-blowing stuff.
Hope you fine 75 minutes to watch, again here: bit.ly/2AiPTmj
Back tomorrow for weekly roundup.
Hope you fine 75 minutes to watch, again here: bit.ly/2AiPTmj
Back tomorrow for weekly roundup.