
1/14 I was always asked as a student if I wanted to give fluids to a patient, but no one ever told me how they think about. Here is my approach to giving IV fluids.
Disclaimer: Things are simplified for the sake of pragmatism.
#MedTwitter #MedEd
Disclaimer: Things are simplified for the sake of pragmatism.
#MedTwitter #MedEd
2/14 I call my approach an "IV fluid timeout." It involves asking yourself four questions before giving someone IV fluids. 
3/14 I broke down the answer two question one into two major buckets. This is the most important question because if a patient does not need IV fluids, do not give IV fluids.
4/14 The approach for intervening directly correlates to one of the major buckets from question 1.
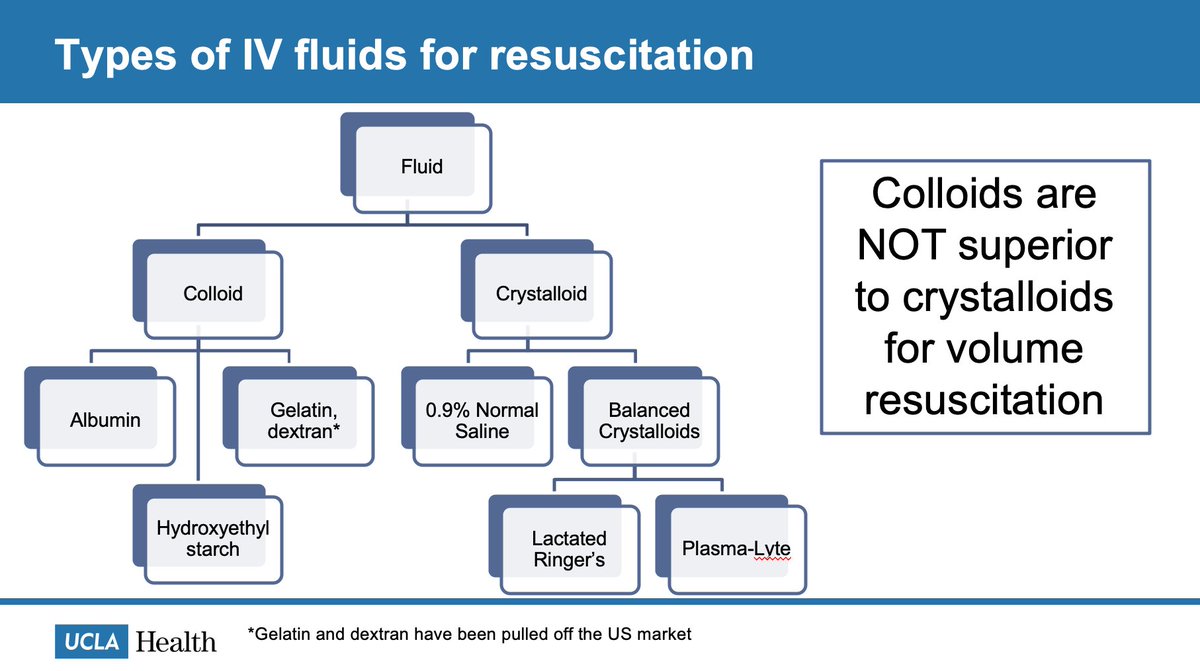
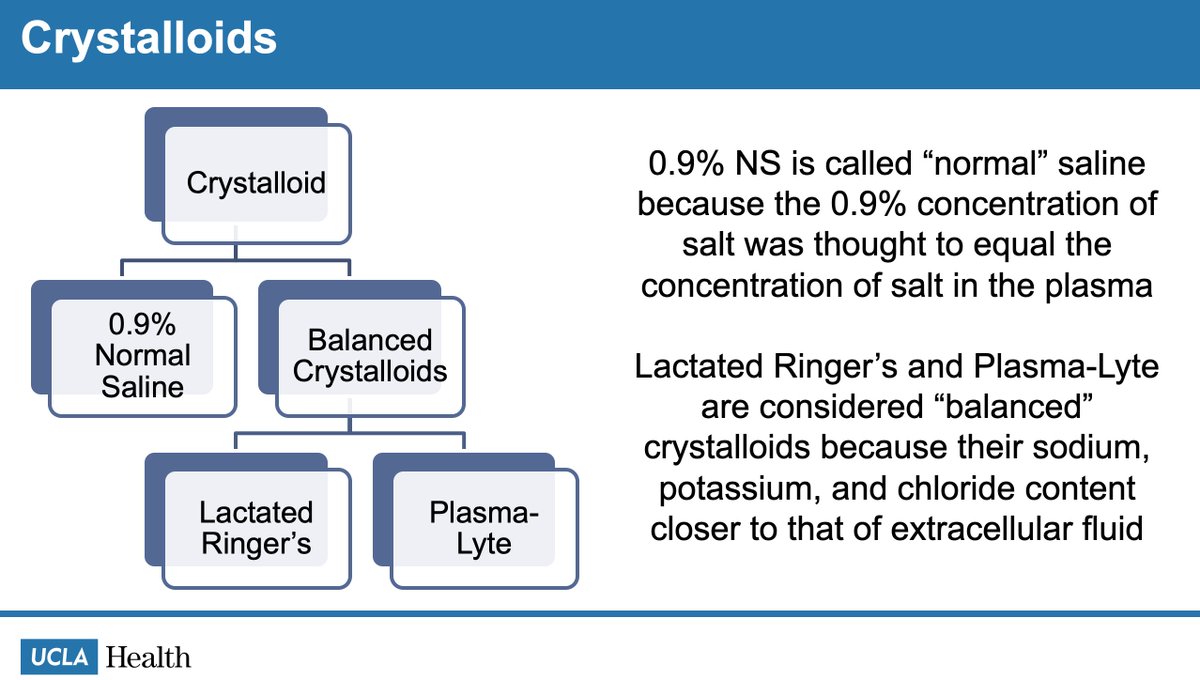
5/14 Now we need to talk about the type of resuscitative fluid to give. First we need to figure out what's in our toolkit (this is NOT comprehensive but what is commonly used).
Colloids not superior to crystalloids for resuscitation! pubmed.ncbi.nlm.nih.gov/30073665/
Colloids not superior to crystalloids for resuscitation! pubmed.ncbi.nlm.nih.gov/30073665/
6/14 These are the most commonly used crystalloids in medicine, however you are allowed to make your own as well.
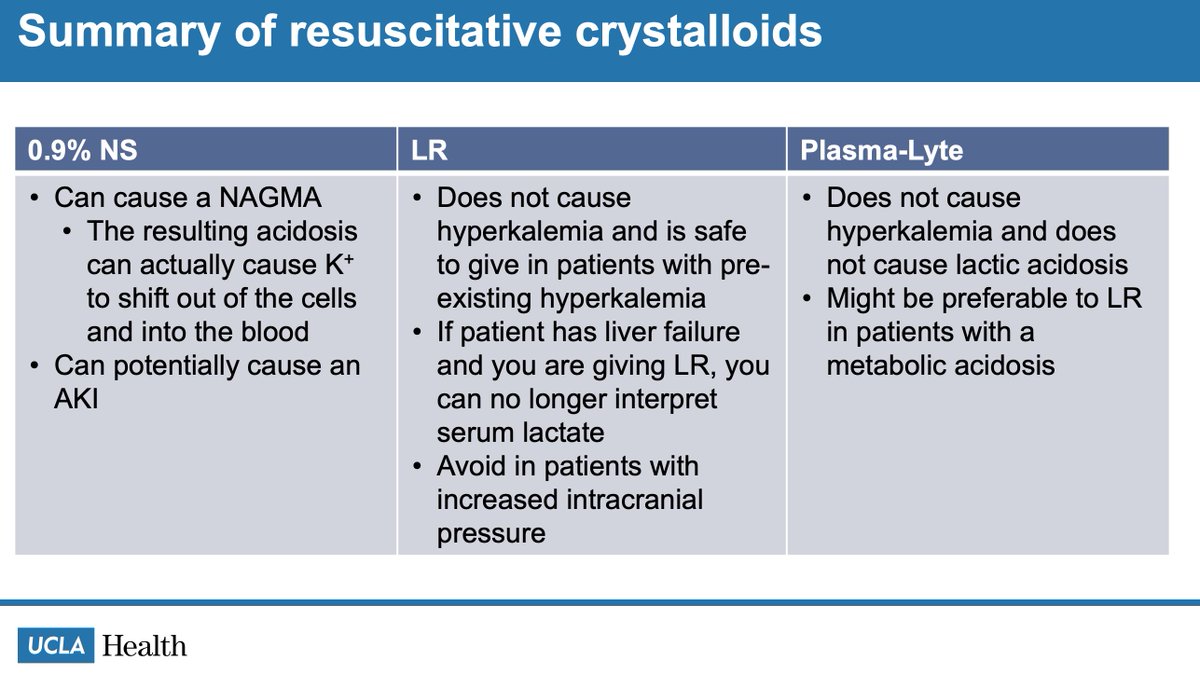
7/14 Let's start by talking about 0.9% NS. It can cause a NAGMA and it can WORSEN hyperkalemia. Thanks @DrKanaris

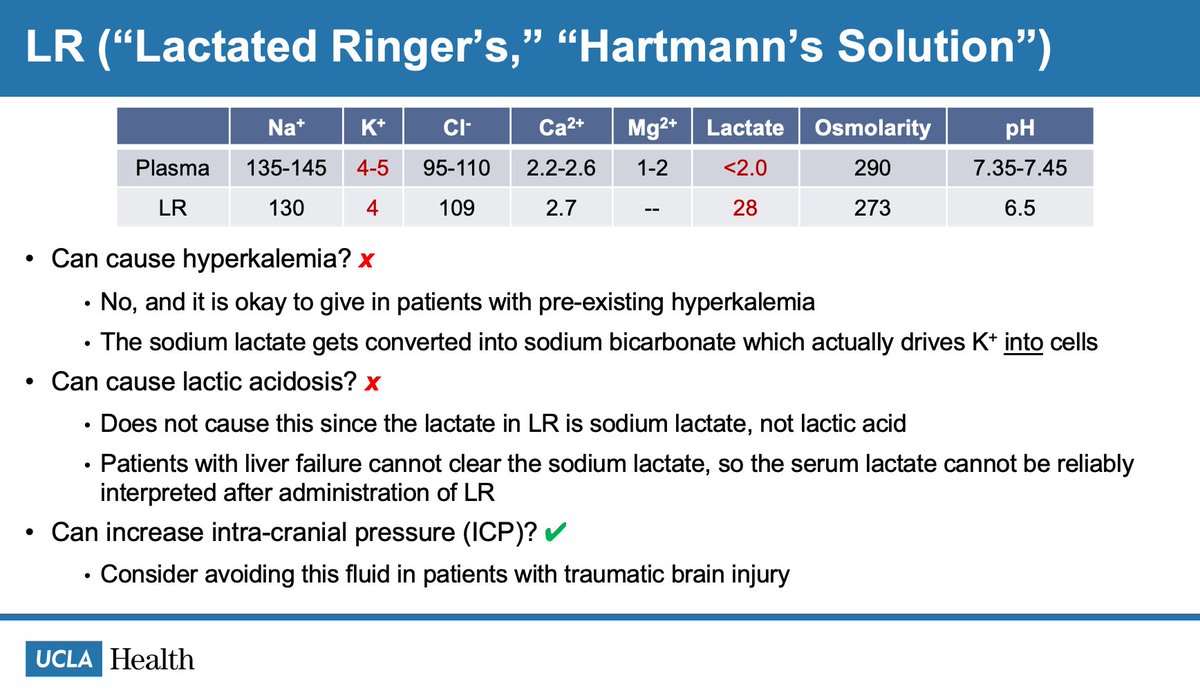
8/14 LR does not cause hyperkalemia. If you choose to trend serum lactate levels, you cannot do so in cirrhotic patients who are receiving LR. LR is hypotonic to plasma and can worsen ICP.
9/14 Plasma-Lyte might be preferable to LR because it has a pH that is closer to that of blood, but the jury is still out.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…

10/14 Here is a summary of the three options that were reviewed.
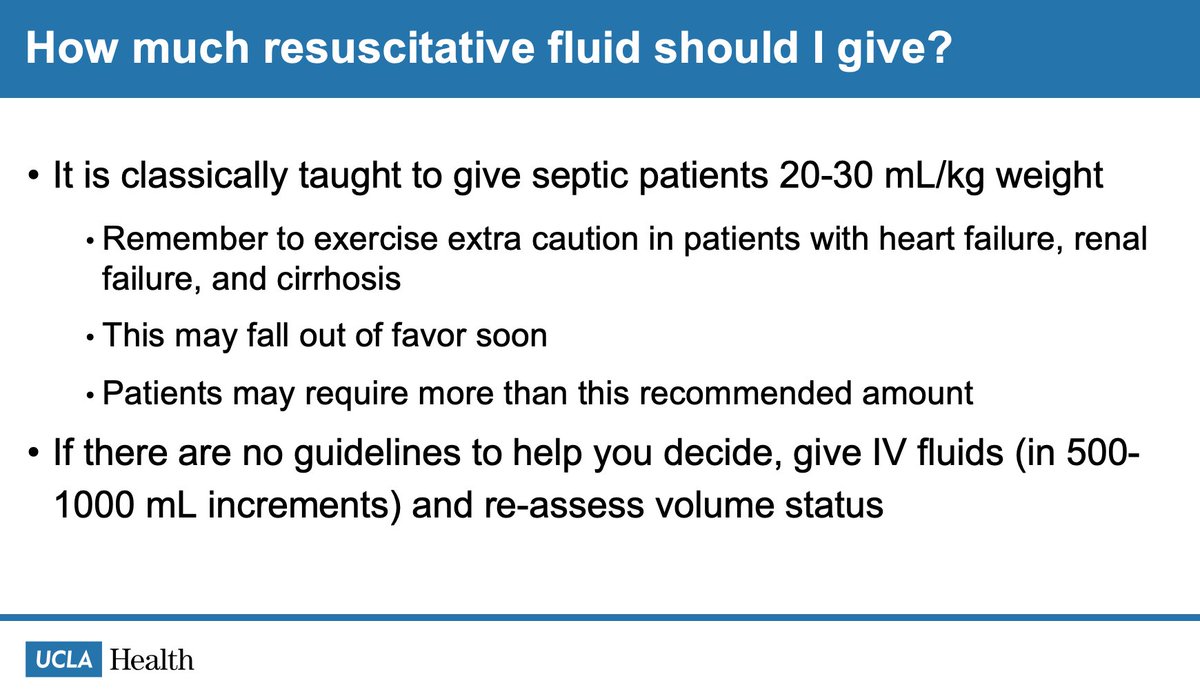
11/14 The amount of fluid to give is highly debated. You will see 20-30 cc/kg for sepsis thrown around. The best answer is to give some amount of fluid (considering the patient's organ's abilities to accommodate the fluid) and reassess (using vitals, exam, and POCUS).
12/14 Let's shift gears to maintenance fluids. 0.45 NS + D5W is a good option (closest tonicity to plasma). There is much debate that the tonicity of the fluid is even relevant. There IS value in having the fluid contain glucose as this can help suppress catabolism.
13/14 Amount of maintenance fluid is calculated using an equation from pediatric literature in 1957. There is debate about this as well, but the calculation does give you a good starting point to decide on the rate.
pubmed.ncbi.nlm.nih.gov/13431307/
pubmed.ncbi.nlm.nih.gov/13431307/

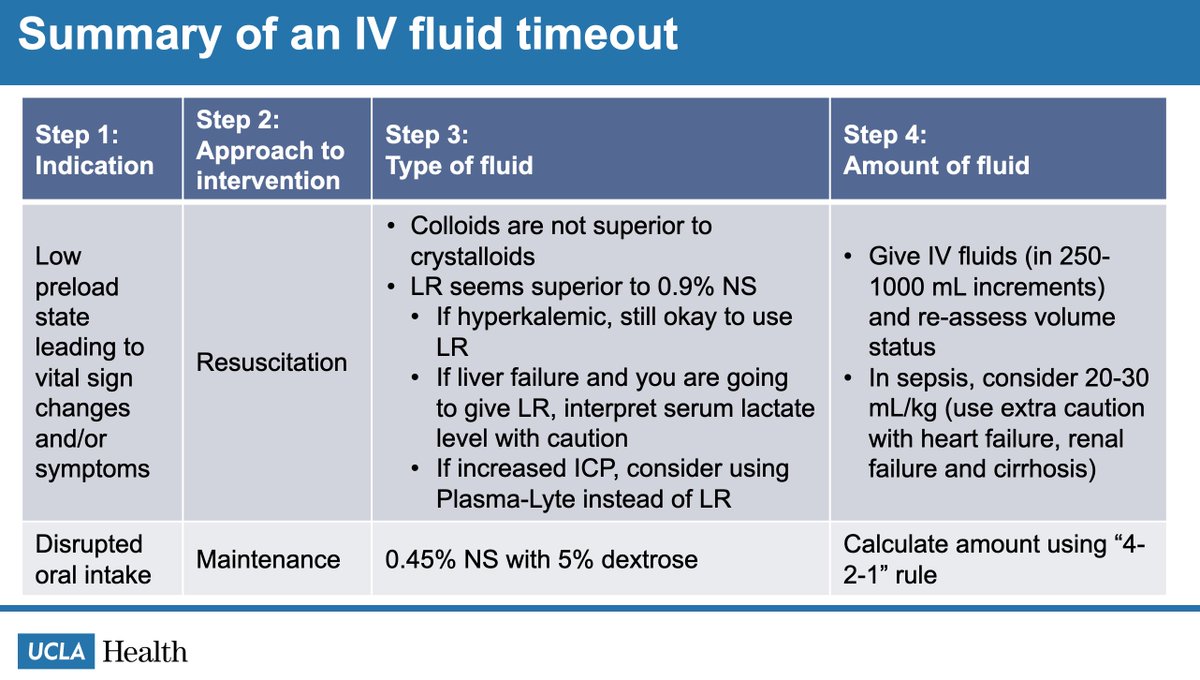
14/14 Here is a summary of an IV fluid timeout. Although it lacks the truest nuance that administration of IV fluid deserves, it is a place to start!
You can use it to diagnose hepatorenal syndrome or to maximize the efficacy of furosemide. Surgeons sometimes prefer it (the rationale for this is beyond my scope as an internist).

