🚨 Multi-part case #Tweetorial
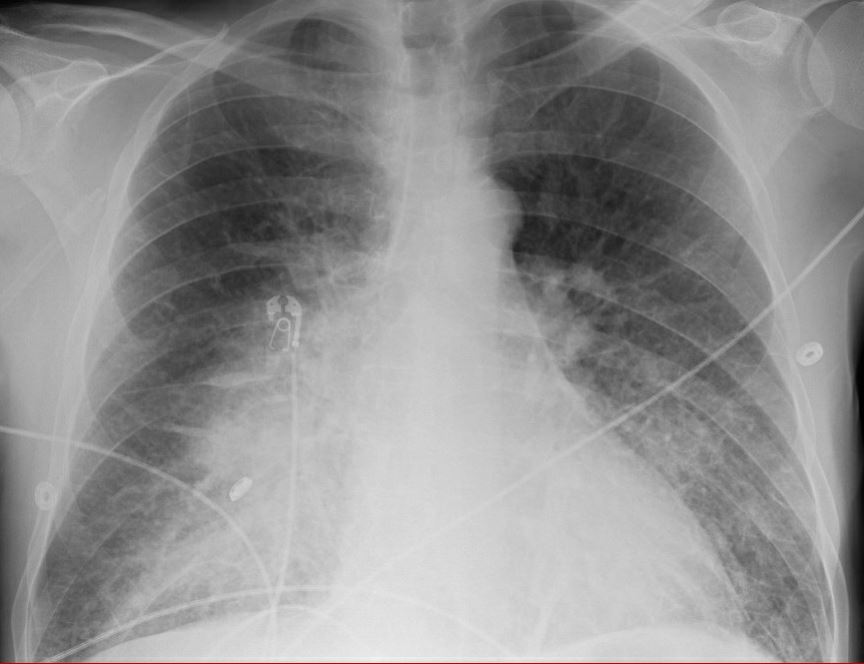
24y man no PMH. 3-4 days myalgias, freq diarrhea. 2L saline given on med floor -> hypox/tachypnea. COVID pend.
A 👍
B RR30-34, SpO2 92% 5L NC
❤️ MAP 90, HR 110s ->150s over 12 hrs
D Avpu
E Anxious
L CRP 58 (ULN 0.9), Cr 1.4 (no baseline), Lact 4.8
24y man no PMH. 3-4 days myalgias, freq diarrhea. 2L saline given on med floor -> hypox/tachypnea. COVID pend.
A 👍
B RR30-34, SpO2 92% 5L NC
❤️ MAP 90, HR 110s ->150s over 12 hrs
D Avpu
E Anxious
L CRP 58 (ULN 0.9), Cr 1.4 (no baseline), Lact 4.8

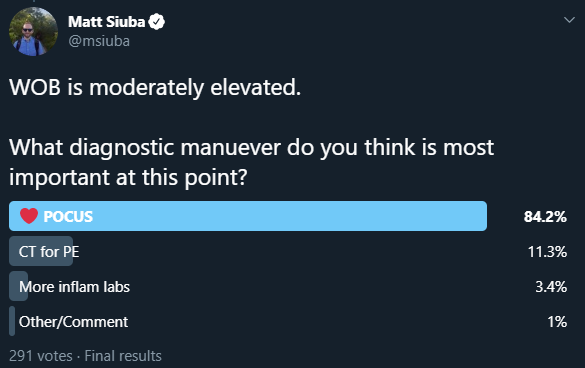
WOB is moderately elevated.
What diagnostic manuever do you think is most important at this point?
What diagnostic manuever do you think is most important at this point?
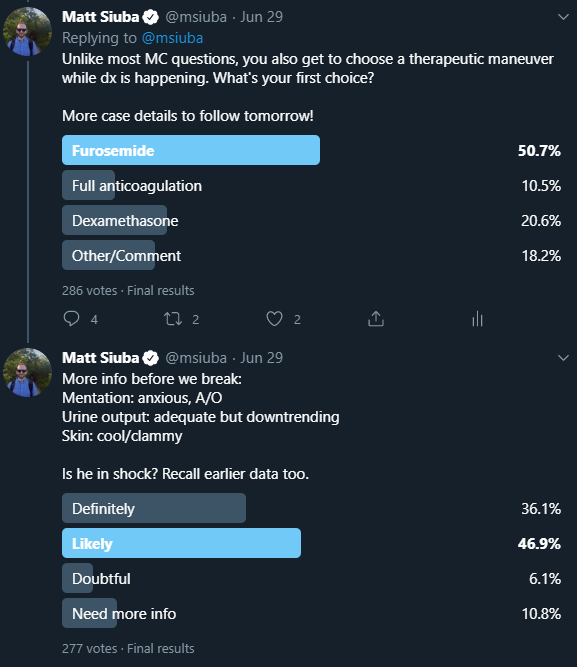
Unlike most MC questions, you also get to choose a therapeutic maneuver while dx is happening. What's your first choice?
More case details to follow tomorrow!
More case details to follow tomorrow!
More info before we break:
Mentation: anxious, A/O
Urine output: adequate but downtrending
Skin: cool/clammy
Is he in shock? Recall earlier data too.
Mentation: anxious, A/O
Urine output: adequate but downtrending
Skin: cool/clammy
Is he in shock? Recall earlier data too.
For those waiting... it's time to resume! (cc @reepRN @emily_fri @Thind888 @mkashiouris @f_g_zampieri @ogi_gajic)
Before you move on in the case, the RN brings you this EKG done for tachycardia. Next step (poll following)?
Before you move on in the case, the RN brings you this EKG done for tachycardia. Next step (poll following)?
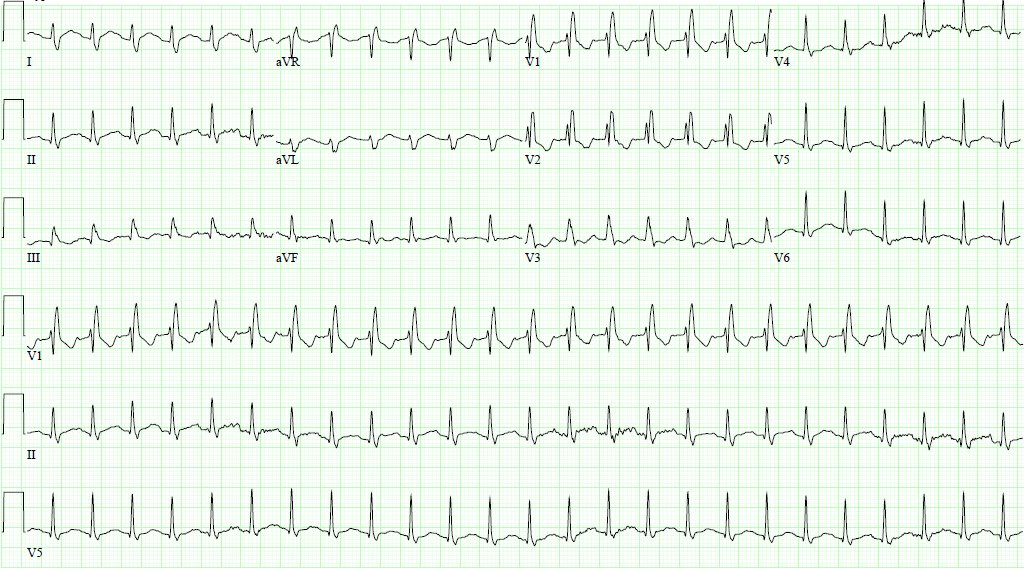
What to do with that EKG in this patient?
Let's also review the poll results from yesterday.
The vast majority felt #POCUS #echofirst was needed, and that, more likely than not, this patient is in shock.
More of a mix for therapeutic choice, but the #DiuresisJedi crew outvoted the steroid crew.
How about that echo?
The vast majority felt #POCUS #echofirst was needed, and that, more likely than not, this patient is in shock.
More of a mix for therapeutic choice, but the #DiuresisJedi crew outvoted the steroid crew.
How about that echo?
What are you expecting to see on echo? Will give a bit of time for poll answers, then we will review images and next steps.
COVID rapid swab is sent. No medications given on the basis of the EKG.
You're starting to worry that this patient's cardiac output might be dependent on the heart rate of 150.
He is progressively anxious, now prefers to sit upright for respiratory comfort.
You're starting to worry that this patient's cardiac output might be dependent on the heart rate of 150.
He is progressively anxious, now prefers to sit upright for respiratory comfort.
As such, the portable #POCUS images you are able to obtain are not optimal, but certainly instructive...
What's the diagnosis?
What's your next step?
Vitals: MAP 100-110, HR 150s, 92% on 5L NC, RR still 30-34
Vitals: MAP 100-110, HR 150s, 92% on 5L NC, RR still 30-34
Many choices here are reasonable, certainly there is room for debate. Would have felt risky to start an intrope at first go, but the other options all have merit depending on your comfort and experience.
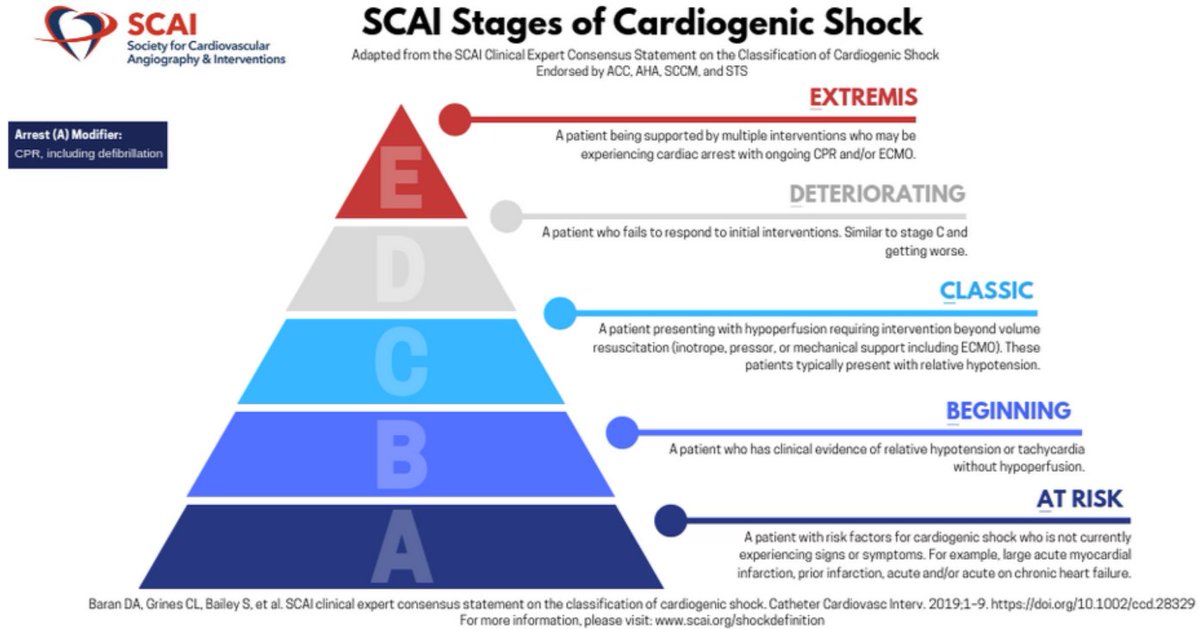
As per SCAI classification, this pt is at least "C", bordering "D"
As per SCAI classification, this pt is at least "C", bordering "D"
To share thought process: this pt was diagnosed overnight in a community hospital ICU.
With near certainty of need for transfer to a dedicated CCU (anticipating possible MCS), a PAC was placed to guide initial mgmt. So 2 answers chosen (help + PAC).
Numbers below:
With near certainty of need for transfer to a dedicated CCU (anticipating possible MCS), a PAC was placed to guide initial mgmt. So 2 answers chosen (help + PAC).
Numbers below:

Calculated CI by Fick is 1.4, estimated SV only 17 cc!
PAPi (measure of RV performance) only 1.25.
More on PAPi here: pubmed.ncbi.nlm.nih.gov/29597051/
Pt has a good deal of MAP room as @Thind888 suggested. As the RN is stringing up nitroprusside, the rapid #COVID19 test comes +
PAPi (measure of RV performance) only 1.25.
More on PAPi here: pubmed.ncbi.nlm.nih.gov/29597051/
Pt has a good deal of MAP room as @Thind888 suggested. As the RN is stringing up nitroprusside, the rapid #COVID19 test comes +
In short, this is #COVID19 myocarditis.
Nitroprusside is pushed to max dose, filling pressures improve a bit, but MvO2 is stable at 48. Lactate still 4.9
Next step?
Nitroprusside is pushed to max dose, filling pressures improve a bit, but MvO2 is stable at 48. Lactate still 4.9
Next step?
Intrope trial wins!
Dobutamine was started at 5 mcg/kg/min, within 5-10 min frequent PVCs/non-sust VT were seen, so dose cut to 2.5.
Over about an hour, HR began to improve to 120s-130s. MvO2 modestly improved to 54.
Dobutamine was started at 5 mcg/kg/min, within 5-10 min frequent PVCs/non-sust VT were seen, so dose cut to 2.5.
Over about an hour, HR began to improve to 120s-130s. MvO2 modestly improved to 54.
Unfortunately he subsequently had several bouts of emesis and developed respiratory distress just prior to transfer.
He was intubated and experienced brief PEA arrest in the aftermath.
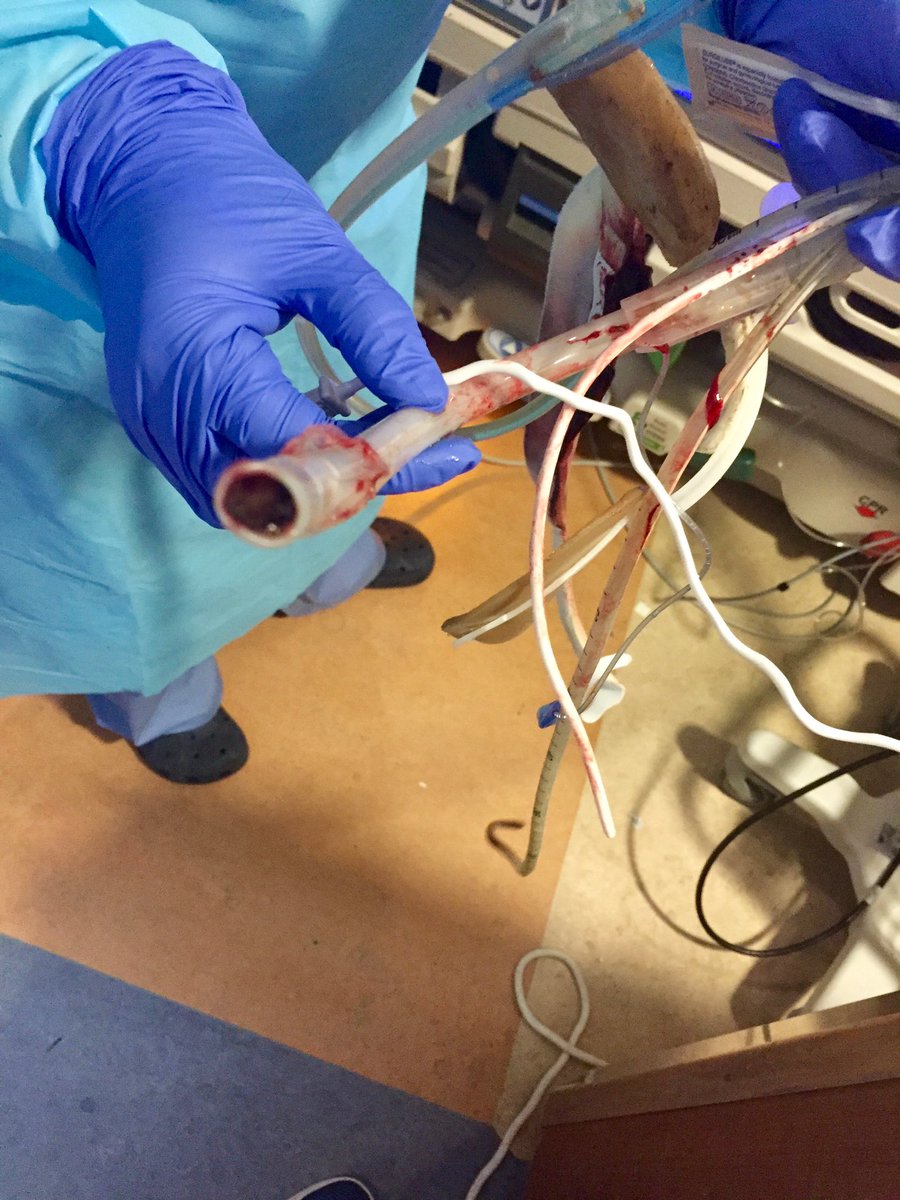
After prompt transfer to CCU, LVEF had fallen to 10%. VA-ECMO and pLVAD were placed quickly
He was intubated and experienced brief PEA arrest in the aftermath.
After prompt transfer to CCU, LVEF had fallen to 10%. VA-ECMO and pLVAD were placed quickly
Fortunately, he was able to be supported without incident on MCS.
After several days, LV/RV function recovered to normal levels. He was decannulated and able to leave the hospital, neurologically intact, within 10 days.
After several days, LV/RV function recovered to normal levels. He was decannulated and able to leave the hospital, neurologically intact, within 10 days.
Admittedly I have no specific expertise on #COVID19 myocarditis.
Here's an ESC video on it from March, which at this point could be considered outdated:
youtube.com/watch?time_con…
Here's an ESC video on it from March, which at this point could be considered outdated:
youtube.com/watch?time_con…
So what are the learning points? 1/x
- It is your obligation as a clinician to explain tachycardia. This patient's cardiac output was completely dependent on it in light of such a low SV. Giving fluids or beta blockade here would have certainly been deleterious.
- It is your obligation as a clinician to explain tachycardia. This patient's cardiac output was completely dependent on it in light of such a low SV. Giving fluids or beta blockade here would have certainly been deleterious.
- Beware clinical history of "dehydration". Aggressive hydration for a history of diarrhea without any objective attempt at volume assessment is problematic at the least.
- Know the resources of your institution, and when someone needs to move out ASAP. Delays can be deadly 2/x
- Know the resources of your institution, and when someone needs to move out ASAP. Delays can be deadly 2/x
- Anxiety is absolutely a diagnosis of exclusion, esp in ICU. There is often a physiologic explanation, (as for tachycardia!).
- If you practice acute care, *please* learn #POCUS. Waiting for formal studies in patients like this is too costly. 3/3
- If you practice acute care, *please* learn #POCUS. Waiting for formal studies in patients like this is too costly. 3/3
@threadreaderapp please unroll