Are we already near the herd immunity threshold for #COVID19 ?
New paper by highly respected Oxford authors is shockingly bad.
Why is #COVID19 making great scientists lose their mind?
Very short thread.
medrxiv.org/content/10.110…
New paper by highly respected Oxford authors is shockingly bad.
Why is #COVID19 making great scientists lose their mind?
Very short thread.
medrxiv.org/content/10.110…
There have been a bunch of recent papers showing that simplistic calculations of the herd immunity threshold (HIT) assuming a "well-mixed" homogenous population produce values that are too high. I wrote a detailed thread about it here:
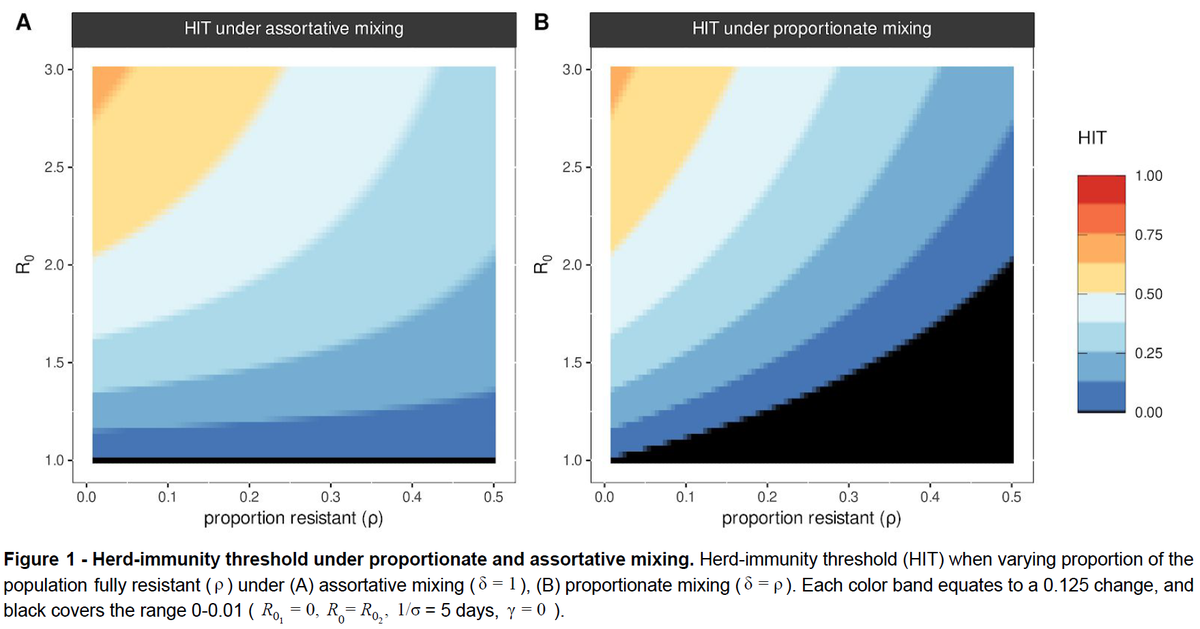
This new paper is downright silly biologically. It assumes some fraction of the human population is fully resistant (i.e. cannot transmit, Rt=0) and shows graphs where this fraction is 50% of population. Then, big surprise, HIT is lower than if everyone is equally susceptible. 
This paper might have been a fun math exercise on a rainy day when we were planning a picnic pre-COVID, but during a pandemic when we have hard data that shows the assumptions of the model to be false is worse than counterproductive. It's Ioannidis' territory bad.
There are plenty of studies showing that the virus has swept through entire households (), and moderate fractions of larger groups of people -NYC- became infected despite societal lockdowns ().
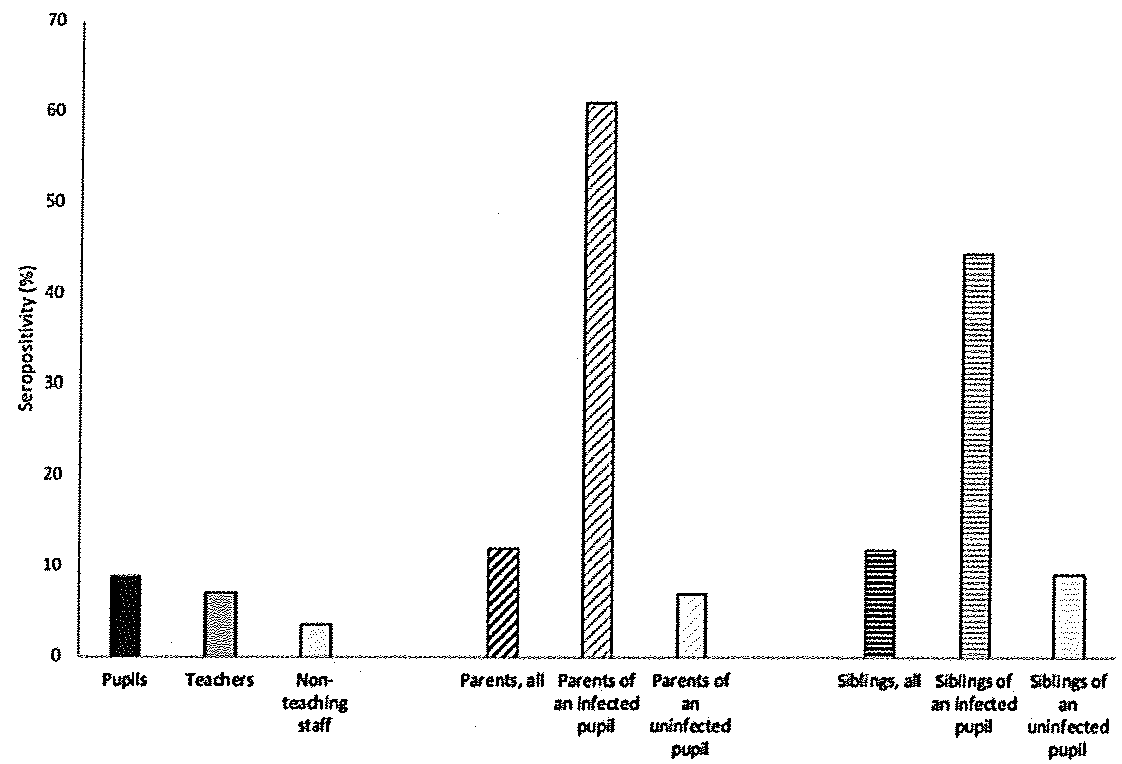
How then is it plausible to suggest that up to 50% of people might be resistant to infection? It's simply nutty.
Authors amazingly conclude that the HIT might be 10% or less. Simply ridiculous. Seroprevalence is >10% in several small-med pops now.
Authors amazingly conclude that the HIT might be 10% or less. Simply ridiculous. Seroprevalence is >10% in several small-med pops now.

Note that this is the same 1st and last authors who proposed back in March that half of UK might already have been infected. Nicer people than me suggested they were just illustrating uncertainties that needed to be addressed with seroprevalence studies.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
This follow up paper suggests they must have some very weird perspective on the world and aren't aware of the voluminous data that makes the assumptions they propose as reasonable clearly false.
Just for clarity (in case you didn't read my detailed thread on HIT: ), I am NOT suggesting that HIT based on homogenous well-mixed models is correct. It is almost certainly an overestimate. But it's unknown whether it is 30% or 40% instead of 60% if R0=2.5
But hard data show it is NOT <10%, and there is no mythical 50% of the pop that is resistant to infection.
Addition: This thread takes a pretty harsh tone & I should be more careful to not make personal attacks. So I'd like to explain with less snarky but still very direct words why this paper is problematic, and why it's even worse that it comes from highly respected people at Oxford
From early on in this epidemic, the biggest challenge has been a reluctance to take swift & substantial actions to limit the epidemic. The pandemic would be hard enough to control if we recognized it for what it was immediately. But we (US, UK, Italy, Spain, Iran, Brazil) didn't.
The reason we didn't act immediately is because many of the larger actions (closing businesses, travel) had huge economic consequences, & if the threat wasn't real, it would be a bad idea to close unnecessarily. So we needed to be sure it would be bad.
(Business closures aren't only way to control #COVID19, as many countries have shown; we can & should be pursuing these alternate approaches. I wrote about this here:
It is the most important thread I've ever written about COVID19. Please share widely.)
It is the most important thread I've ever written about COVID19. Please share widely.)
Early questions about COVID threat were less about transmissibility of virus & more about deadliness. Early work showed that reproductive rate, Rt, of virus was at least 2 & in some places might be 3-5, w/ a generation time of 3-7d. Infections could clearly grow very fast.
There was huge early debate about the fatality of #COVID19, primarily because of uncertainty about the fraction of infections that were asymptomatic, and confusion about the case vs infection fatality rate (CFR & IFR). I wrote about this here:
There are now multiple rigorous estimates of age-specific IFR that correct for delays, test inaccuracies, etc. based on serological data or closed pops that make it very clear that COVID is deadly (>10x higher than seasonal flu (). Pop. IFR ~0.5-1.5%
For those wanting to dig into flu vs COVID deadliness here's a nice detailed article by @GidMK
link.medium.com/tmJQWautc8
link.medium.com/tmJQWautc8
Debate has now shifted about what fraction of people are likely to get infected if we don't shut down businesses. This discussion involves both the herd immunity threshold (HIT) and "overshoot". I wrote a detailed thread about HIT & overshoot before:
This is essentially a return to the discussion of "should we (continue) to close businesses?". If we are at or near HIT, then transmission will be lower & we don't need to close businesses. But if we aren't then cases will rise again, and more rapidly if Rt>>1.
Cases are rising rapidly in many US states and countries around the world despite some mask use & social distancing recommendations, so it's clear we're nowhere near HIT in these places. NYT separates states by increasing vs decreasing. Almost all are inc.

Despite this, many US states (and countries) still do not take rapid action to slow transmission. Businesses in which transmission risk is high & cannot be made safe (e.g. bars) are still open. People think its safe to gather. Masks are still recommended but not required.
When papers like the Oxford study are published they offer a smokescreen for politicians to stand behind while their citizens become sick & die when they could have taken action to protect them (& their jobs: ).
The fact that authors are very well-respected & from Oxford makes it much easier for politicians to claim the pandemic is almost over and we should just "try to get through it".
Mathematical models have played a unique role in this pandemic in showing us how bad things can get (& how quickly) if we don't take swift action. Models like the Oxford study do the reverse. They suggest - against all evidence - that we can do nothing and infections won't rise.
The opposite is clearly true. The skyrocketing cases and associated rising deaths (that come a month later) are clear proof that we are nowhere near herd immunity and to suggest otherwise is both patently false and dangerous.
The flawed science in this preprint will be used to justify actions that cost peoples' lives & continued transmission that hurts the economy & society. The authors are very intelligent people employed by a highly respected institution, and they should know better.
So while I sincerely apologize for tone in tweets above that came across as a snarky personal attack, I strongly stand behind my criticisms of both the flawed science and the lack of responsibility on the authors' part.