What is the actual likelihood of aerosol transmission?
This is a much-discussed question with huge consequences.
A fantastic new paper has actual data to address the question by monitoring infection in nurses caring for #COVID19 patients.
Thread.
medrxiv.org/content/10.110…
This is a much-discussed question with huge consequences.
A fantastic new paper has actual data to address the question by monitoring infection in nurses caring for #COVID19 patients.
Thread.
medrxiv.org/content/10.110…
Background
A huge question with any new pathogen is:
How is it transmitted?
SARS-COV-2 is a respiratory virus and *could* be transmitted by surface contamination, close-range contact via large droplets, & longer distance via smaller aerosol particles.
A huge question with any new pathogen is:
How is it transmitted?
SARS-COV-2 is a respiratory virus and *could* be transmitted by surface contamination, close-range contact via large droplets, & longer distance via smaller aerosol particles.
I wrote detailed thread on this before and will summarize key points again here.
It matters b/c it determines how we stop transmission. If surface contamination was major mechanism then avoiding touching frequently-touched surfaces and hand-washing/hygiene would be key. This was suspected to be important in March & led to 20+ sec hand-washing campaign.
Extensive data have shown it rarely is the source of transmission (CDC website & quote below).
cdc.gov/coronavirus/20…
I know of only 1 *possible* case of surface transmission:
So, handwashing=good in general, but not much help for COVID.
cdc.gov/coronavirus/20…
I know of only 1 *possible* case of surface transmission:
So, handwashing=good in general, but not much help for COVID.

If transmission is entirely by large droplets, then keeping 6' away and wearing loose masks (surgical, cloth) will prevent most of transmission, and indoor activities would be safe.
If aerosol transmission is possible or likely, then much tougher to stop transmission. Need more ventilation, tighter fitting and better (more expensive N95 masks), and indoor activities (dining, movies, etc.) much higher risk even w/ masks and distance.
Epidemiological data has shown that MOST transmission can be explained by close-range contact. But not ALL of it. A few cases suggest longer range spread. See thread for careful analysis of each example:
But past data were all just anecdotes. What we needed was larger sample size of either observational data or experiments. @Babak_Javid_Lab had clever ideas about having infected people in room and using animal models to measure transmission. Maybe he can re-link to tweet.
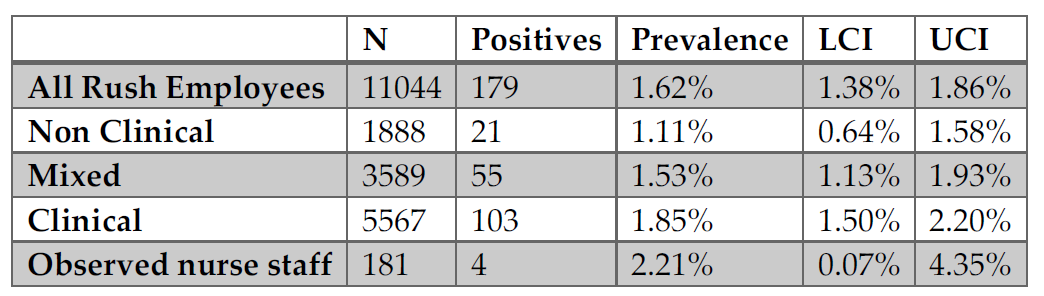
This study is even better (but still with limitations). They measured infection in 181 health-care-workers (HCWs) in 1198 interactions lasting 19503 min total (16.3 min each) w/ 152 unmasked infected patients. HCWs wore mostly surgical masks.
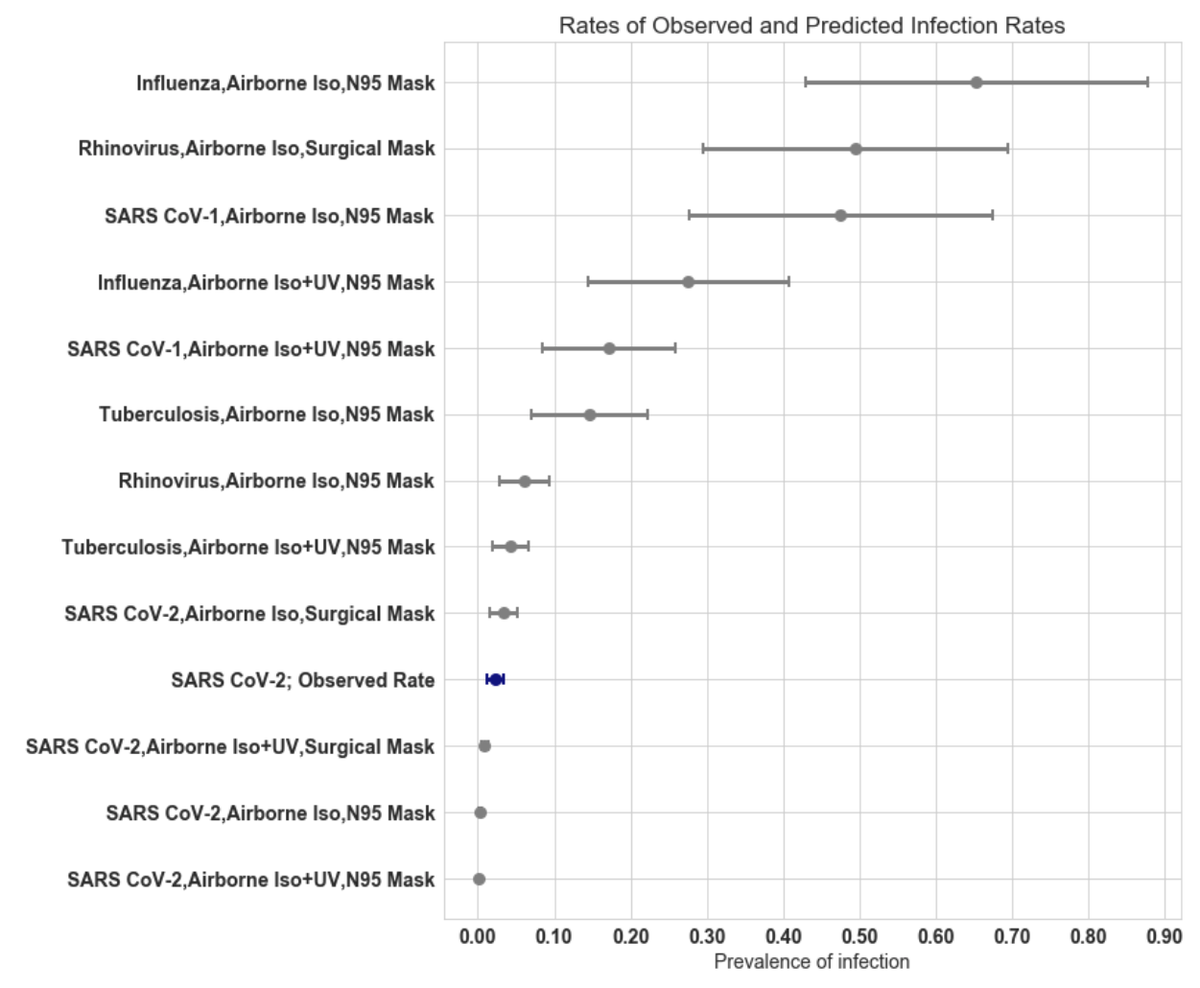
They found that 4/181 health care workers got infected & used mathematical model to estimate risk of infection & compared to other viruses w/ previous data. Aerosol risk MUCH lower than other viruses & TB.
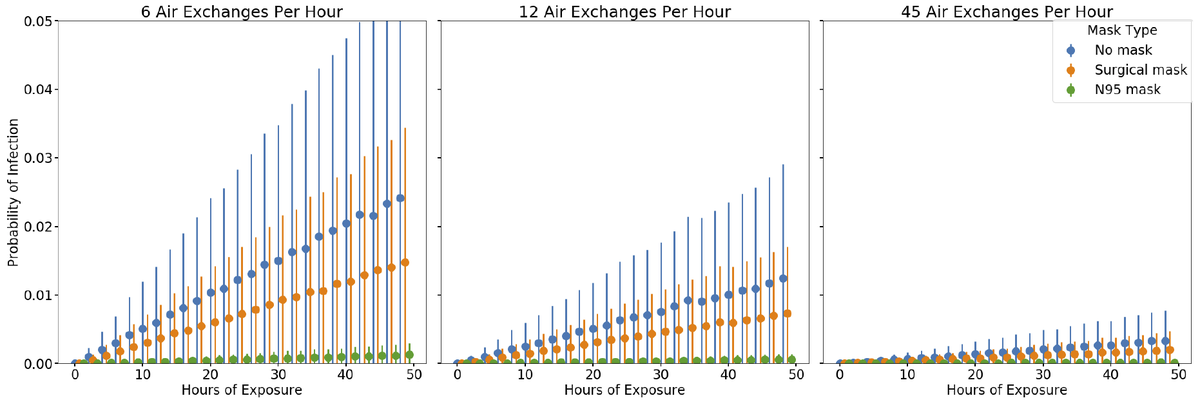
Paper also uses model to examine prob infection vs ventilation, duration of exposure & mask type. As expected ventilation & duration of exposure make huge diff. Surgical mask just a bit.
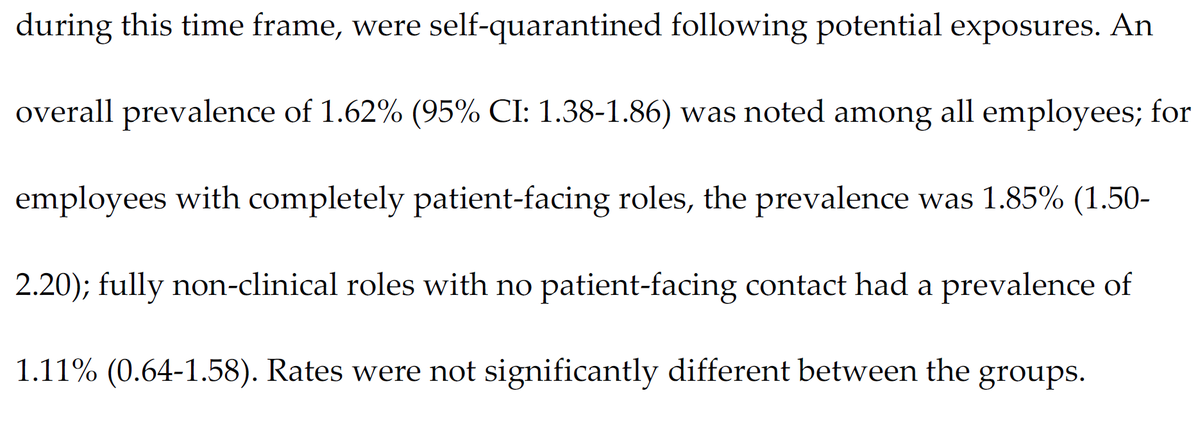
Additional Details: prevalence in HCWs working w/ COVID patients was slightly higher than those not working w/ patients.
What do these data indicate?
Authors conclude: "Overall, our findings suggest that SARS-CoV-2 is not well transmitted via the airborne route in controlled conditions"
This provides hard data to back up earlier indirect assessments based on epidemiological investigations.
Authors conclude: "Overall, our findings suggest that SARS-CoV-2 is not well transmitted via the airborne route in controlled conditions"
This provides hard data to back up earlier indirect assessments based on epidemiological investigations.
Caveats
-Infected people were patients and infectiousness decays over time, so pre-symptomatic person might produce more virus. See thread:
-4 HCWs could have become infected from droplets not aerosols.
-Infected people were patients and infectiousness decays over time, so pre-symptomatic person might produce more virus. See thread:
-4 HCWs could have become infected from droplets not aerosols.
My Conclusions:
-Aerosol transmission *can* occur (as we knew before)
-It does NOT happen often (as we suspected)
-Ventilation helps a bunch (which we suspected)
-Masks help (which we knew)
-Aerosol transmission *can* occur (as we knew before)
-It does NOT happen often (as we suspected)
-Ventilation helps a bunch (which we suspected)
-Masks help (which we knew)
Translation:
Being indoors w/ an infected person (who may not know it!) with poor ventilation & no masks is a bad idea!
Being indoors w/ an infected person (who may not know it!) with poor ventilation & no masks is a bad idea!
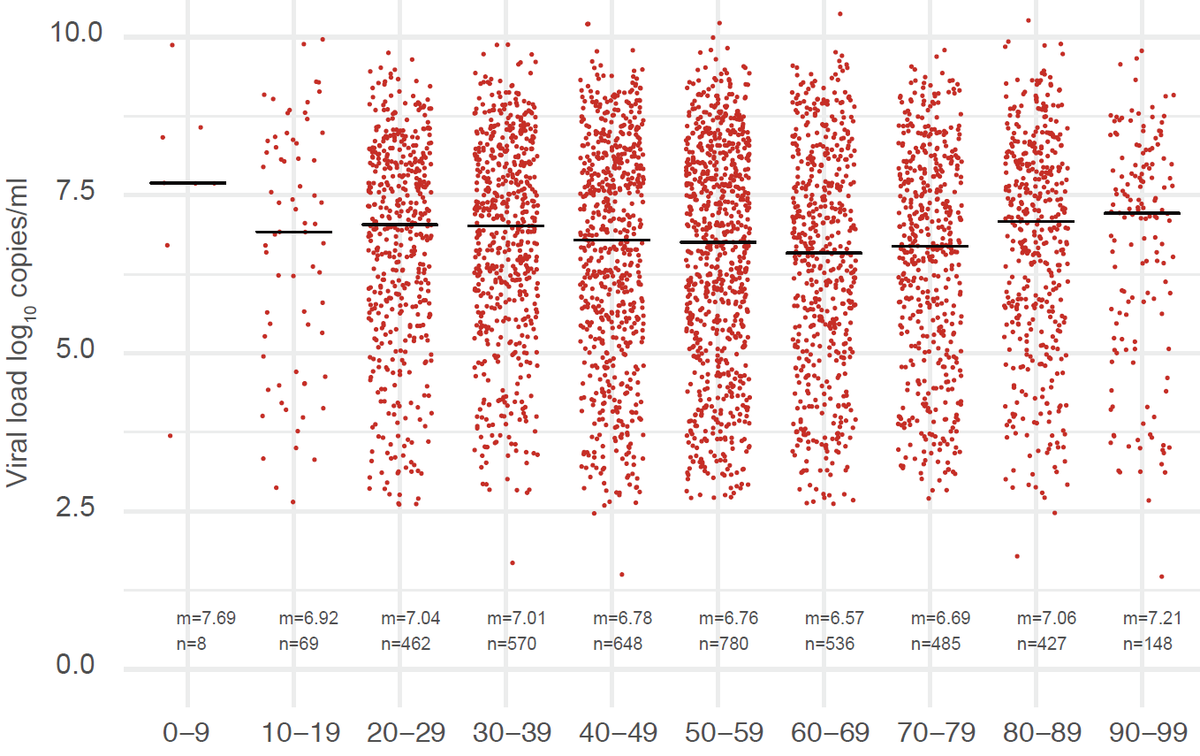
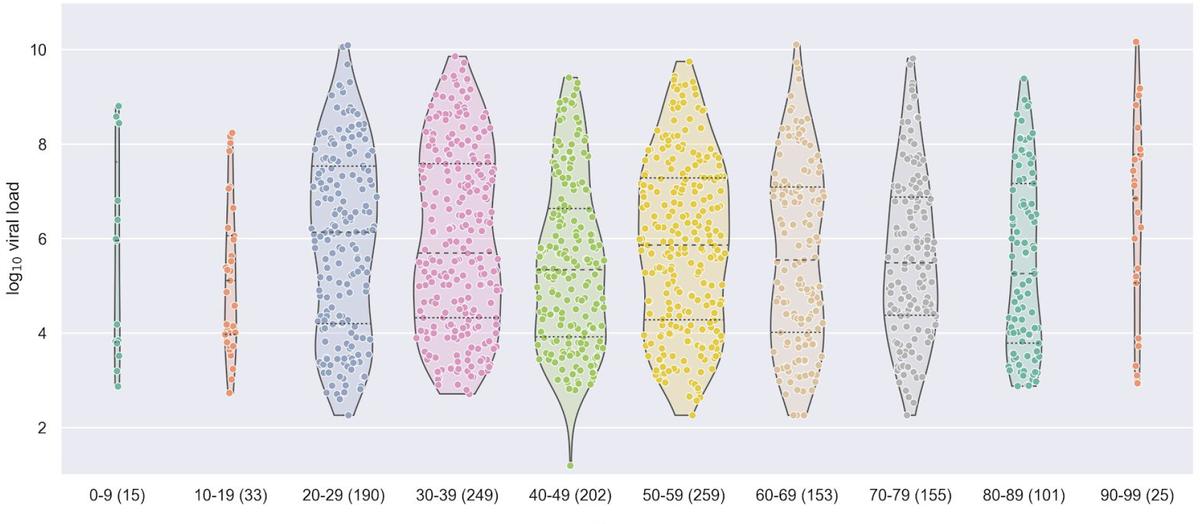
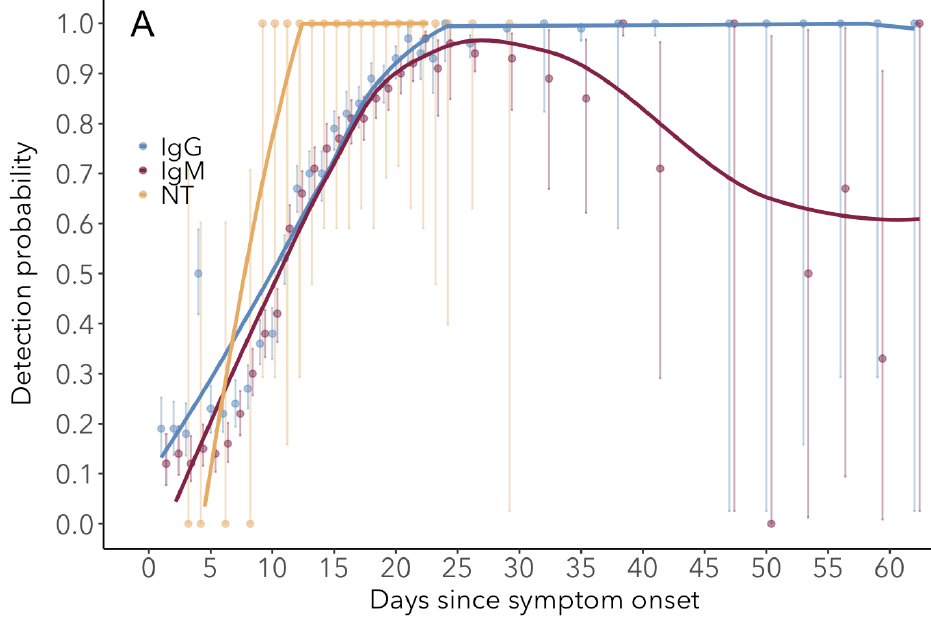
Remaining questions: How does aerosol risk vary w/ viral load of infected person (no data shown) & thus days since infection ().
Is risk mitigated enough by ventilation & masks to allow indoor dining, theaters? Need epi data from these settings!
Is risk mitigated enough by ventilation & masks to allow indoor dining, theaters? Need epi data from these settings!
Coda: There is an absolutely silly thread (that I won't link to) being shared a bunch suggesting that aerosol is responsible for 50% of transmission. This data (and mountains of epidemiological data) suggests that is not the case.
Add. caveats
-Some HCWs could have already been infected before study, but likely not too many given time of study (March) in IL (few cases by then)
-Infections only include symptomatic (for all groups compared), so all are underestimates; wouldn't change qualitative conclusions
-Some HCWs could have already been infected before study, but likely not too many given time of study (March) in IL (few cases by then)
-Infections only include symptomatic (for all groups compared), so all are underestimates; wouldn't change qualitative conclusions
@BalaHota please clarify or comment if I've gotten anything wrong! Nice work!