What?
1. Nutrition 🥩
2. Potassium 🍌
3. Acid base 🧪
4. Phosphorus 🦴
5. Fluid balance 💧
1. Nutrition 🥩
2. Potassium 🍌
3. Acid base 🧪
4. Phosphorus 🦴
5. Fluid balance 💧
💥Nutrition💥
During the development of #AKI solutes acumulate & BUN becomes the most evident solute
BUN rises from a mixture of kidney reabsorption, low GFR, muscle catabolism & protein in diet, resulting in a (+) nitrogen balance
During the development of #AKI solutes acumulate & BUN becomes the most evident solute
BUN rises from a mixture of kidney reabsorption, low GFR, muscle catabolism & protein in diet, resulting in a (+) nitrogen balance
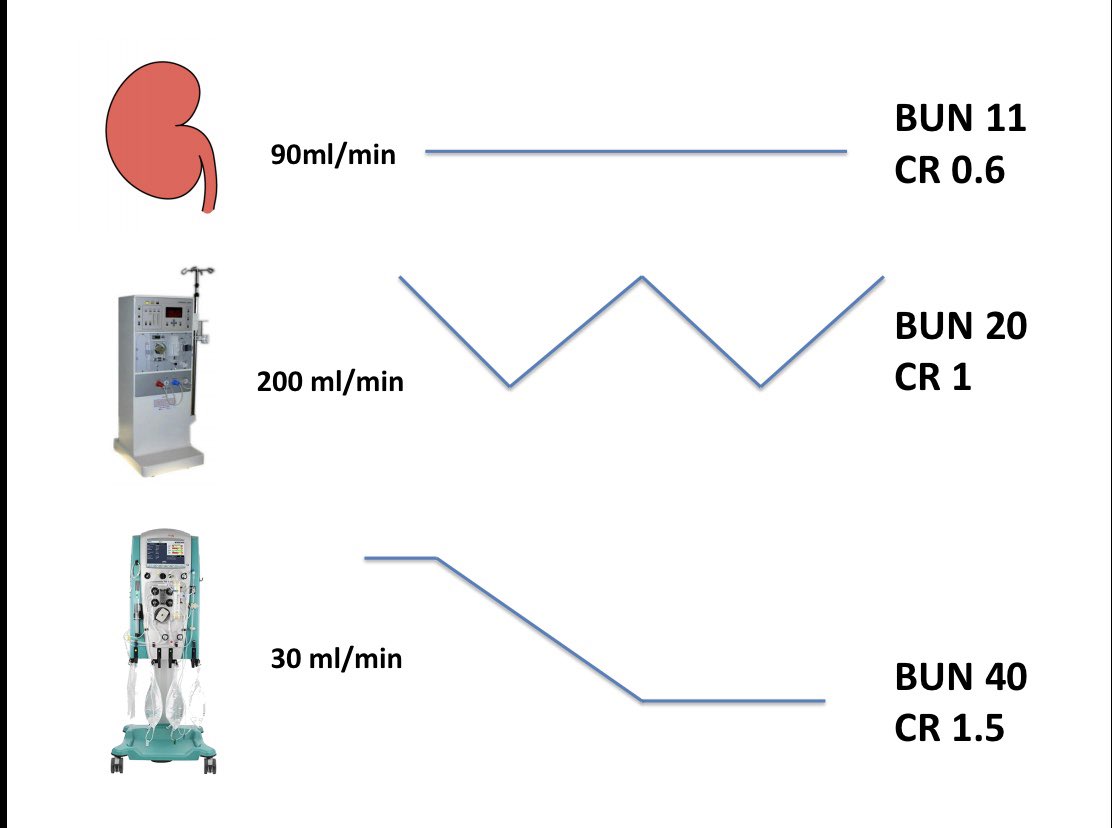
When starting #KRT an initial negative nitrogen balance is expected.
If high catabolism & protein intake are present, there will be a later:
- rebound in intermittent therapies
- steady state in continious therapies
If high catabolism & protein intake are present, there will be a later:
- rebound in intermittent therapies
- steady state in continious therapies
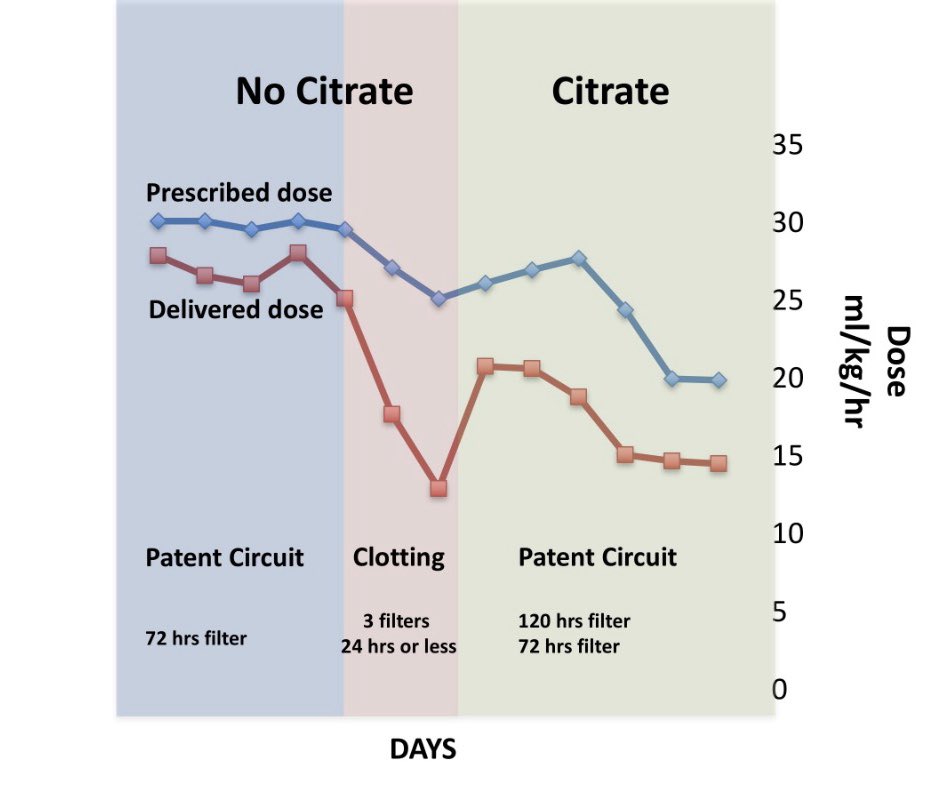
A case using continuous therapy:
2 week #CKRT ➡️ 3 relevant episodes
1. “No citrate” with circuit patency
2. “No citrate” without corcuit patency and significant lower deliverd dose
3. “Citrate” with circuit patency
Prescribed Vs Delivered
2 week #CKRT ➡️ 3 relevant episodes
1. “No citrate” with circuit patency
2. “No citrate” without corcuit patency and significant lower deliverd dose
3. “Citrate” with circuit patency
Prescribed Vs Delivered
1️⃣ The traditional 20-25 ml/kg/hr in #CKRT dose is simply the amount of effluent needed in most patients to achieve the initial (-) nitrogen balance
This number does not fit for every case, should not be a goal, and by any way remain static
This number does not fit for every case, should not be a goal, and by any way remain static
Protein amount should be enough to cover circuit losses & catabolism
-1.5-2.5g/kg/day ~
#CKRT dose should be titrated to mantain a steady state while giving adequate amount of protein.
Don’t forget oligo elements & vitamins
The case 👇
-1.5-2.5g/kg/day ~
#CKRT dose should be titrated to mantain a steady state while giving adequate amount of protein.
Don’t forget oligo elements & vitamins
The case 👇
💥Nutrition💥
1. Initial (-) Nitrogen Balance
2. Steady state
3. Lost of steady state (lost of circuit)
4. Recovery and new steady state
1. Initial (-) Nitrogen Balance
2. Steady state
3. Lost of steady state (lost of circuit)
4. Recovery and new steady state

💥Potassium💥
-Initial: negative balance
-Later: 4K bags + Nutrition mantained a “steady state” no need for replacement
-potassium lowers: replace & reassessment of nutrition & dose
-Initial: negative balance
-Later: 4K bags + Nutrition mantained a “steady state” no need for replacement
-potassium lowers: replace & reassessment of nutrition & dose

💥Phosphorus💥
- Bags don’t have phosphorus so its expected to have a negative balance after 48 hrs, If initial levels are high just like the case, it may take more time.
- Bags don’t have phosphorus so its expected to have a negative balance after 48 hrs, If initial levels are high just like the case, it may take more time.

💥Bicarbonate💥
-35 HCO3 bags during no citrate
-22 HCO3 bags + 12 mmol/hr load of citrate
Works just fine to mantain bicar in steady levels
Nothing to do with lactic & respiratory acidosis
-35 HCO3 bags during no citrate
-22 HCO3 bags + 12 mmol/hr load of citrate
Works just fine to mantain bicar in steady levels
Nothing to do with lactic & respiratory acidosis


If solute control is the goal why bother with DOSING? Well
1️⃣You need to start with something
2️⃣If things are flowing, you need to stablish where you’re standing
3️⃣Monitoring deliverd dose will identify problems related to circuit vs high patient requirements
1️⃣You need to start with something
2️⃣If things are flowing, you need to stablish where you’re standing
3️⃣Monitoring deliverd dose will identify problems related to circuit vs high patient requirements
Last thoughts
1️⃣ Do #KRT with what ever you have avialable & adapt it to your patient to achieve solute control
2️⃣ Timing, dosing & modality should be chosen to achieve solute control
3️⃣ Feed your patient
4️⃣ Know your tools i.e. If using CKRT circuit patency is the priority
1️⃣ Do #KRT with what ever you have avialable & adapt it to your patient to achieve solute control
2️⃣ Timing, dosing & modality should be chosen to achieve solute control
3️⃣ Feed your patient
4️⃣ Know your tools i.e. If using CKRT circuit patency is the priority