Rampant #COVID spread in a kids camp: a preview of school re-opening?
New paper with unsettling details that unfortunately challenges claims that transmission in young children will be lower than adults.
More useful info on %asymptomatic too!
Thread
cdc.gov/mmwr/volumes/6…
New paper with unsettling details that unfortunately challenges claims that transmission in young children will be lower than adults.
More useful info on %asymptomatic too!
Thread
cdc.gov/mmwr/volumes/6…
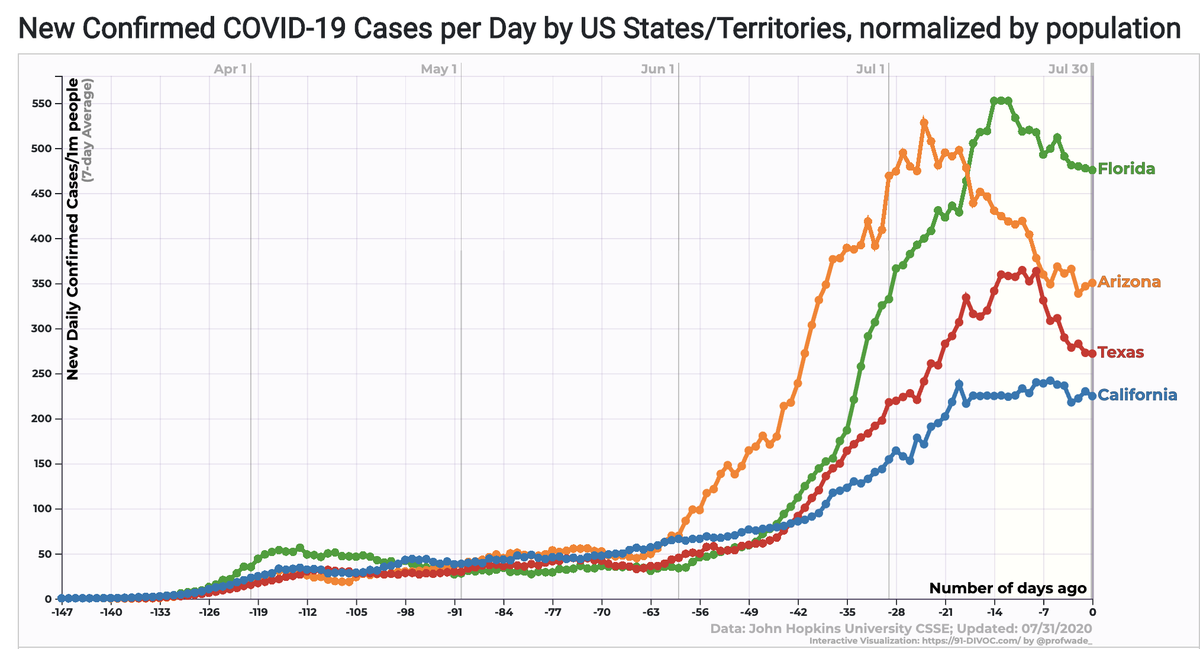
One of the most important outstanding questions in COVID19 epidemiology is how school re-opening will contribute to community transmission. Here's a thread w/ the two contrasting positions:
Schools haven't re-opened in most of the US yet so we're not sure how it will play out. But there have been summer camps in many places. These give us a possible window into what might happen, with the caveat that camps are overnight & have some different activities than schools.
Some activities are riskier (many campers overnight in single cabins) but some are safer (campers often do lots of activities outdoors). So take what happened w/ a grain of salt. But some details are very important.
Study: 258 staff & trainees gathered in GA for 4 days after all had had a negative swab test in previous 12 days. A one time - test up to 12d ago is not an effective screening method:
This thread suggests slightly better approach.
This thread suggests slightly better approach.
After 4 days (Jun 21), 134 trainees left & 346 campers joined 117 staff for 6 more days for a total of 463 people. More than half of campers were <=12; almost everyone was <21. Everyone stayed in cabins, w/ most in large cabins w/ 16-26 people. 
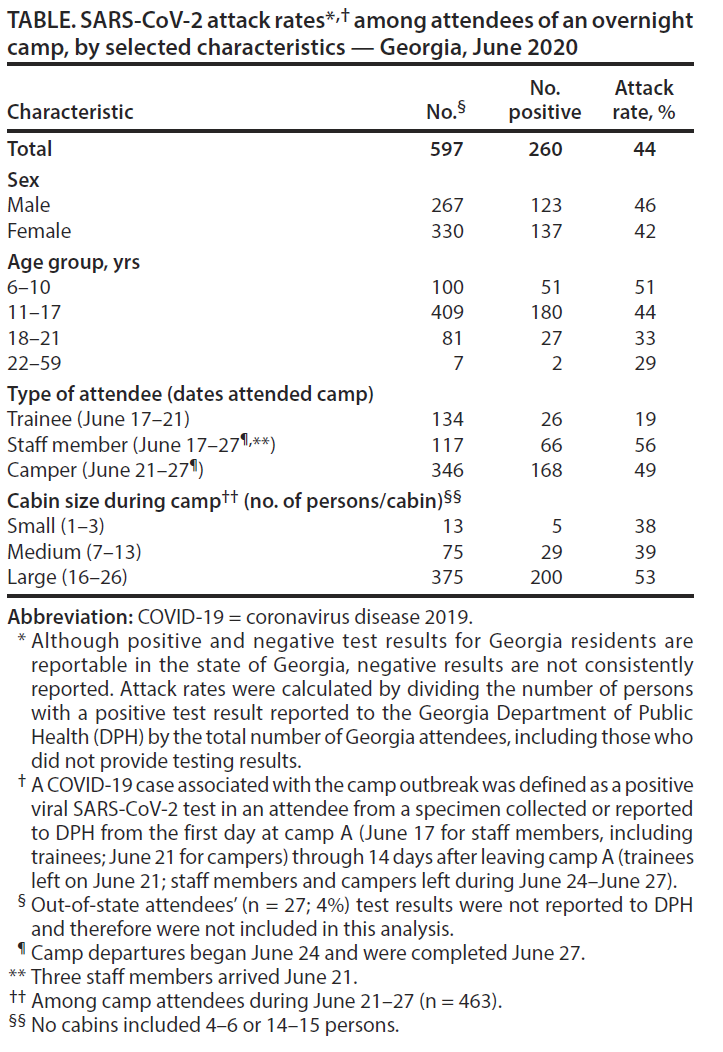
1st case detected was teenage (14-19yr) staff member who developed chills on 3rd day (June 23) after campers arrived. Got tested & got results in 24 hr (fast turn around! Yay!). Camp started sending campers home that day (Jun 24) & everyone gone by June 27.
So total time campers spent at camp was <6d & many <4d. What fraction were infected during this time? 51% of 6-10yr; 44% 11–17 years; 33% 18–21. Yikes. Staff (present whole time 11d): 56%; Trainees (present 4d before campers 19%). Only 26% asymptomatic but mild. So what happened?
Seems pretty clear that 1+staff or trainee came to camp infected (or else 1+ infected campers infected 19% of 134 trainees on 1d of overlap; uncertain how much interaction occurred b/w trainees & campers; seems improbable to me but I wasn't at camp :-)).
Transmission likely occurred within staff/trainees before camp arrival & clearly spread efficiently through campers after they arrived so that 49% were infected in 3-6 days. This time period is so short that at most there was 1 chain of transmission w/in campers.
Note that we still don't know exactly how quickly after infection you are infectious. Best estimates are that, on average, you get infectious 2-3d later & sick 2-3 after that but data are mostly based on adults & v. limited data on viral loads pre-onset:
Since 1st case was detected 3d after campers arrival, if kids were infected on 1st day after arrival (likely) these campers would have just barely had time to become infectious & spread to other campers. Higher probability that most transmission was staff -> campers.
So how did transmission staff->campers occur & how can we prevent recurrence? Article says staff members but not kids had to wear cloth masks (but no info on compliance). Masks wouldn't have been worn when sleeping but not clear if campers slept w/ staff or in separate cabins.
Campers were kept in cabin cohorts, but cabin windows & doors were NOT kept open for ventilation & article mentions "a variety of indoor and outdoor activities, including daily vigorous singing and cheering".
My guess is transmission occurred among staff/trainees during initial 4d pre-camp period leading to many (19%) of trainees & staff infected (but not yet sick). These staff then did most of transmission to campers (with smaller late contribution of campers->campers).
What can (& can't) we conclude?
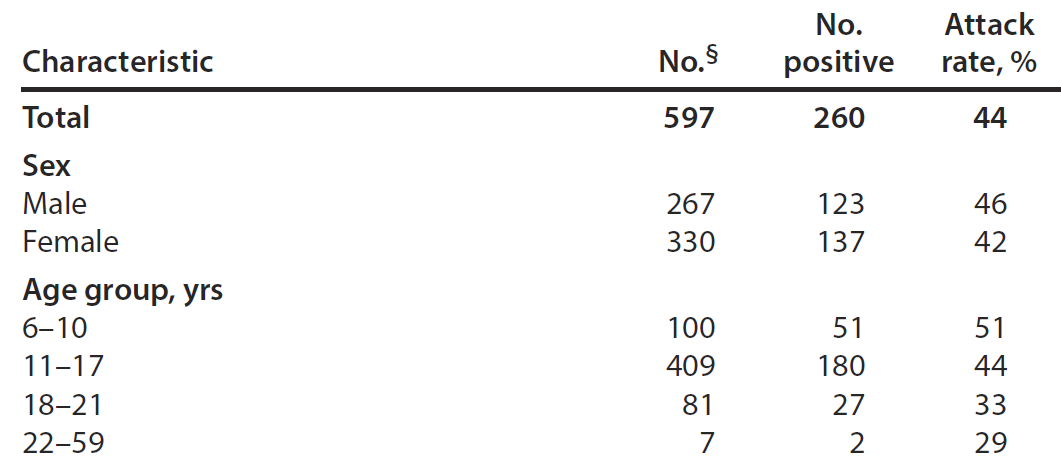
1st: Susceptibility. There have been v strong statements that 0-9 are ~50% as susceptible as 10-19 & adults ( & ). This outbreak is at odds w/ that finding. Attack rate 0-9 >=11-17 (OR 1.16; 0.8-1.7).
1st: Susceptibility. There have been v strong statements that 0-9 are ~50% as susceptible as 10-19 & adults ( & ). This outbreak is at odds w/ that finding. Attack rate 0-9 >=11-17 (OR 1.16; 0.8-1.7).
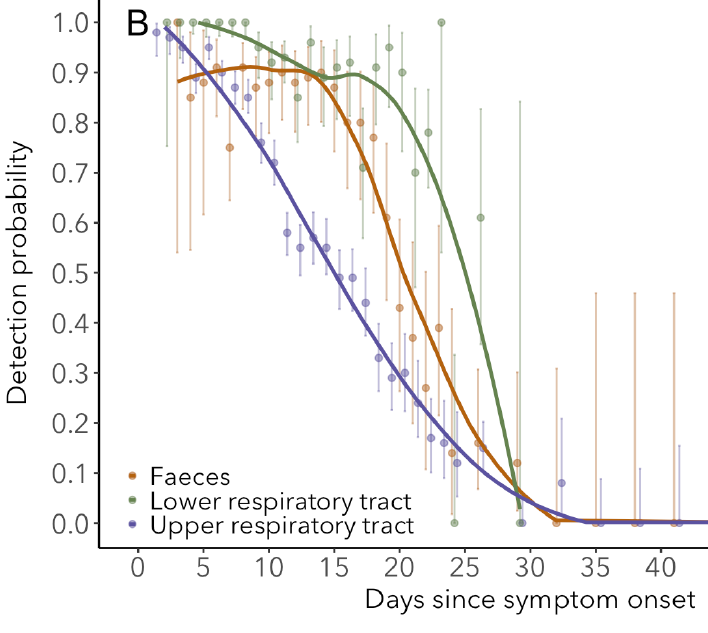
Why are results different here than in household studies? My #1 guess: no bias in timing of testing different people in chain of transmission. If you detect infection in household only after symptomatic case you often miss kids as index case & test after they've cleared virus.
Here that didn't happen - all ages were tested within short time after all infections (exact details sadly not reported in paper but likely done w/in 1 wk after infection when test sensitivity is 90+%
medrxiv.org/content/10.110…)
medrxiv.org/content/10.110…)
2nd possible reason: differences in contact rates
Given sample size here, in order to claim that 6-10 are 50% less susc. than 11-17 you'd have to argue that contact rates were much(!!) higher b/w 11-17 & 6-10 than within 11-17 year olds OR 6-10 kids transmitted to each other.
Given sample size here, in order to claim that 6-10 are 50% less susc. than 11-17 you'd have to argue that contact rates were much(!!) higher b/w 11-17 & 6-10 than within 11-17 year olds OR 6-10 kids transmitted to each other.
I think transmiss. w/in 6-10 is unlikely (see above).
In contrast it is possible that transmission here followed unusual non-age assortative (within age mixing) pattern - i.e. predominantly from already infected staff to kids & not b/w staff after camp started due to cohorting.
In contrast it is possible that transmission here followed unusual non-age assortative (within age mixing) pattern - i.e. predominantly from already infected staff to kids & not b/w staff after camp started due to cohorting.
This would have to make up for fact that staff were present for longer period & had slightly higher attack rate than campers (56 vs 49%; P=0.41). Possible, but contact patterns would have had to be very disparate (very high staff->campers; very low staff->staff).
Most importantly to me, this outbreak shows that we can see very different attack rate patterns w/ age than seen in (biased) household studies. Diffs in attack rates reflect either differences in contact rates OR differences in susceptibility (equal or higher in 6-10 than 11-17).
Critically, we can't tell from measuring attack rates! They do not allow us to separate the two. I cannot emphasize this enough. Would need details on contact rates/duration/type to separate & I've never seen this in household study & it's not presented here.
I *don't* think we can conclude that young kids 6-10 did much of the transmitting here. We don't know if they would have if they had stayed longer, but given the very short time young kids were together, the data is more consistent with spread from 14-21 yr old staff to 0-9 kids.
Clearly rampant spread can happen within kids. Need more activities outdoors, more ventilation indoors (sometimes tough if too hot/cold/rainy/etc.), more space (& masks for kids?) when yelling/cheering. I hope schools will use this lesson in what can happen w/out being careful.
Quick addition: as @mikha_ehl points out, rough prev of infectious people in GA at time was ~1%; suggests ~3 campers came infectious. As detailed above, these could have spread to others in cohort but only time for 1 generation of transmission in campers (most had 4-5d together).
Clarification to last tweet. N=~3 infected/infectious campers would be in addition to the ~20% of 100 (N=20) of staff already infected by start of camp. So, as described above, evidence suggests most infection staff>camper & less camper->camper.