#cardiotwitter #ACCFIT Let's simplify temporary mechanical support!
Slides from Dr. Hussain's talk at #CVBootcamp2020
Think:
💡Is MCS choice appropriate for clinical scenario?
💡Understand and frequently monitor connections & hemodynamics
💡Understand potential complications
Slides from Dr. Hussain's talk at #CVBootcamp2020
Think:
💡Is MCS choice appropriate for clinical scenario?
💡Understand and frequently monitor connections & hemodynamics
💡Understand potential complications
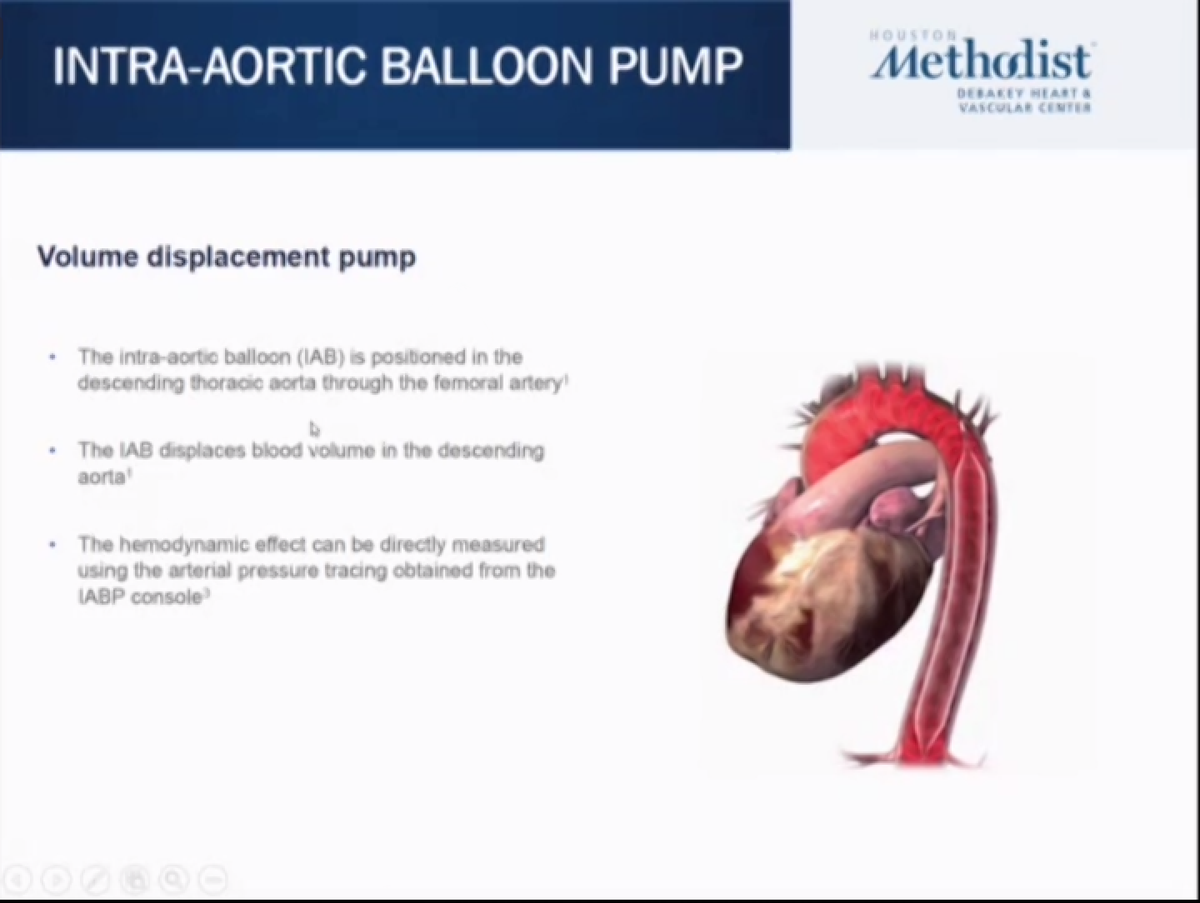
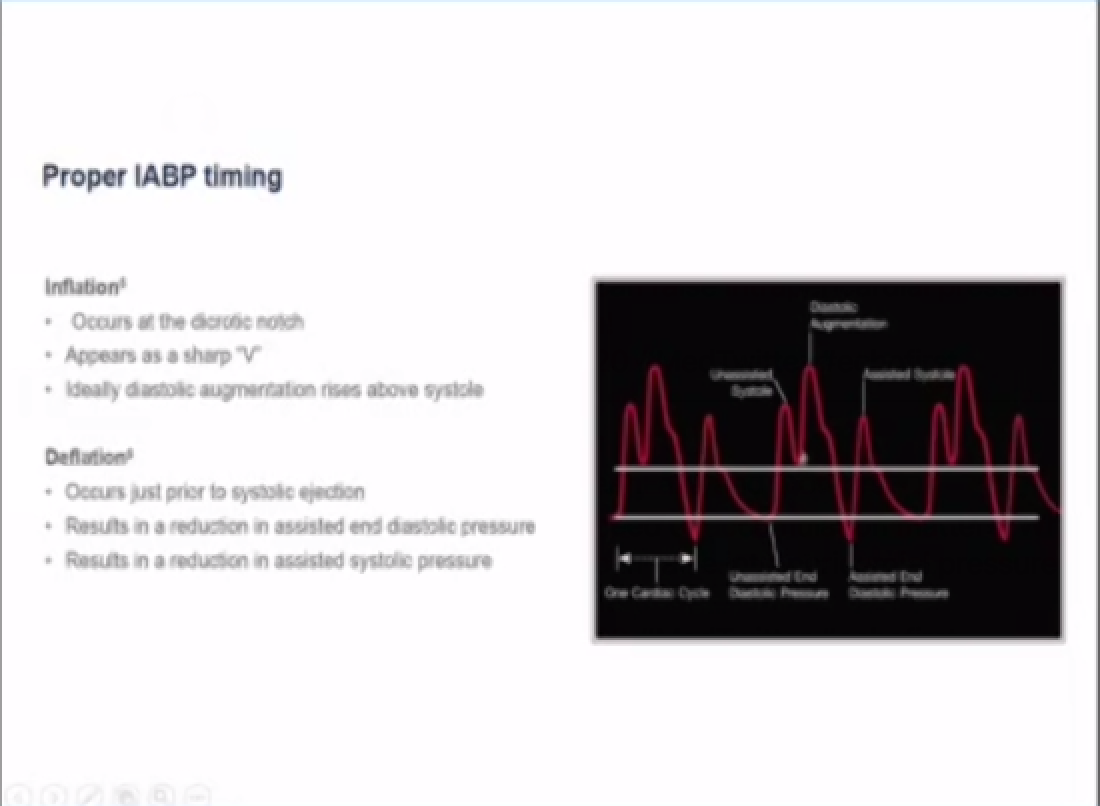
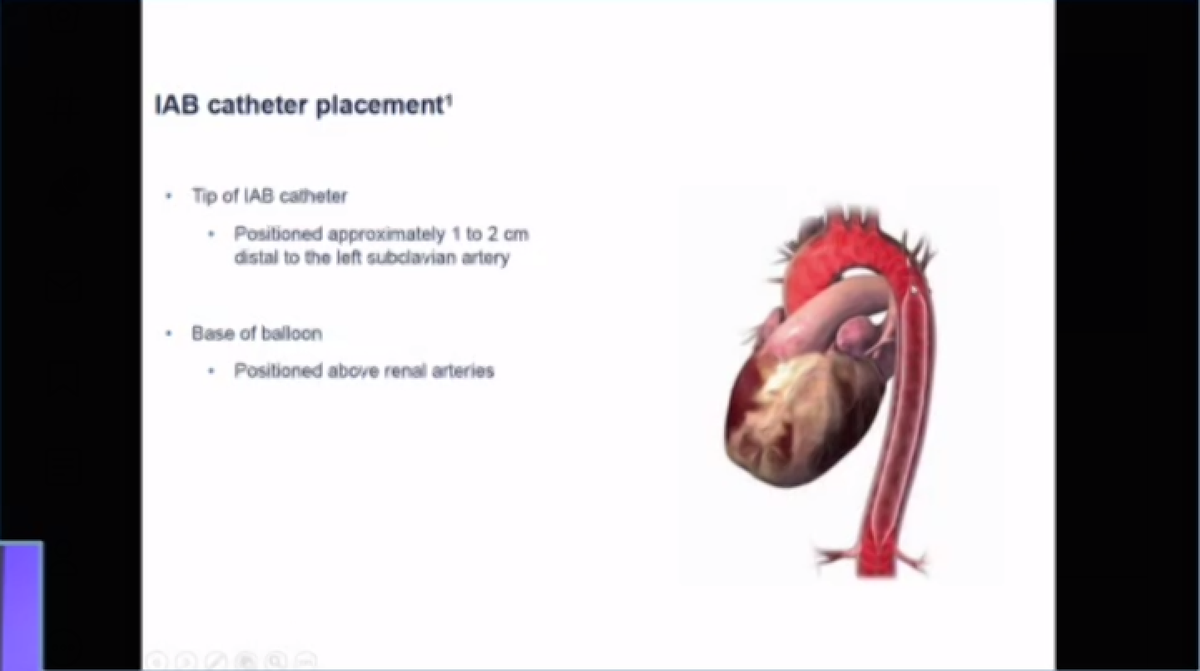
Intra-aortic balloon pump
💡Diastolic augmentation, ⬆️ MAP during augmented beat
💡⬇️ afterload and end-diastolic pressure
💡CO augmentation 0.7-1.4 l/min
💡Position: IABP tip at carina level on CXR
💡Diastolic augmentation, ⬆️ MAP during augmented beat
💡⬇️ afterload and end-diastolic pressure
💡CO augmentation 0.7-1.4 l/min
💡Position: IABP tip at carina level on CXR

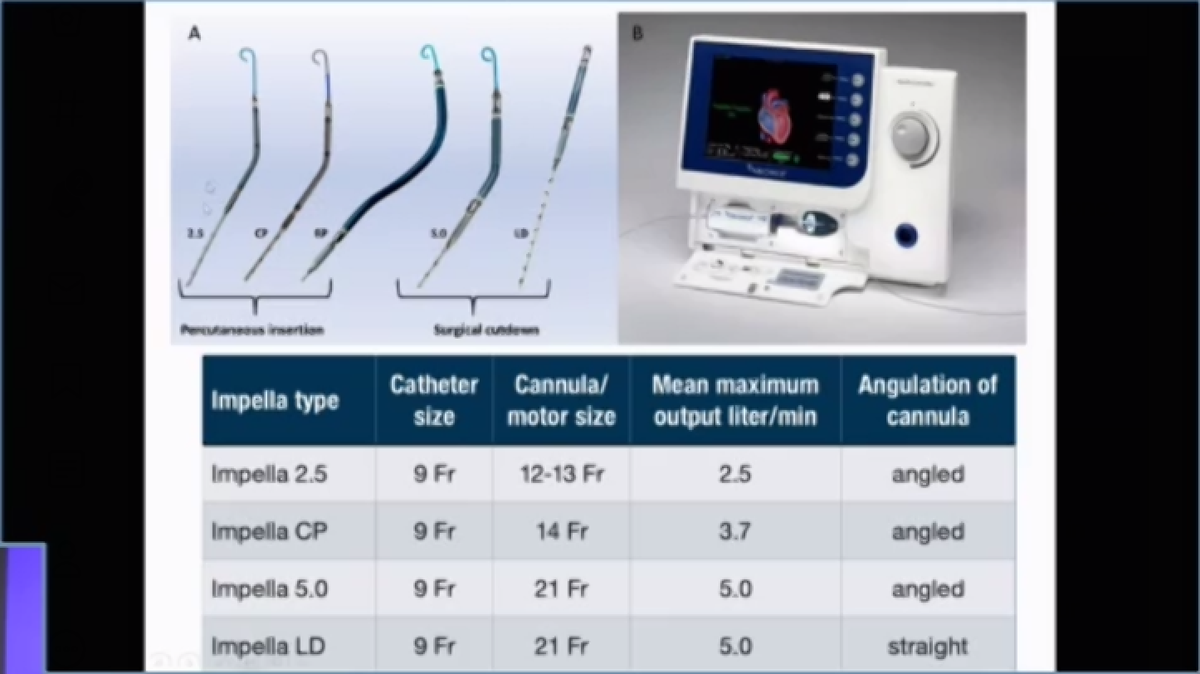
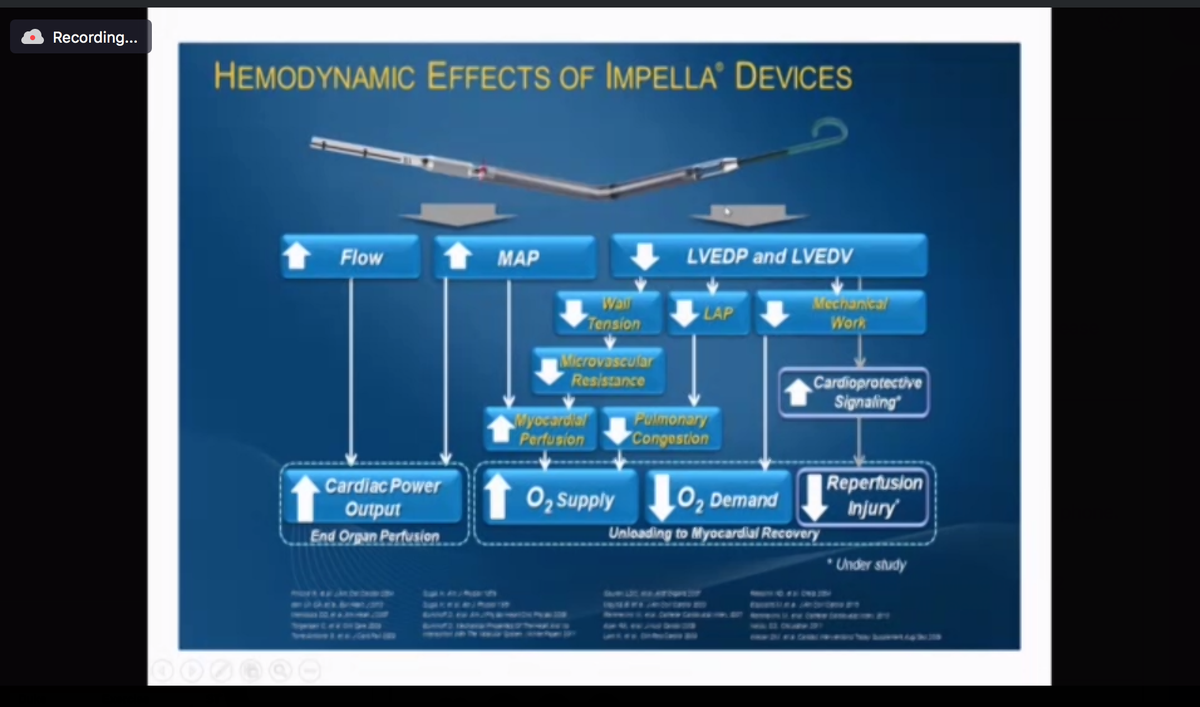
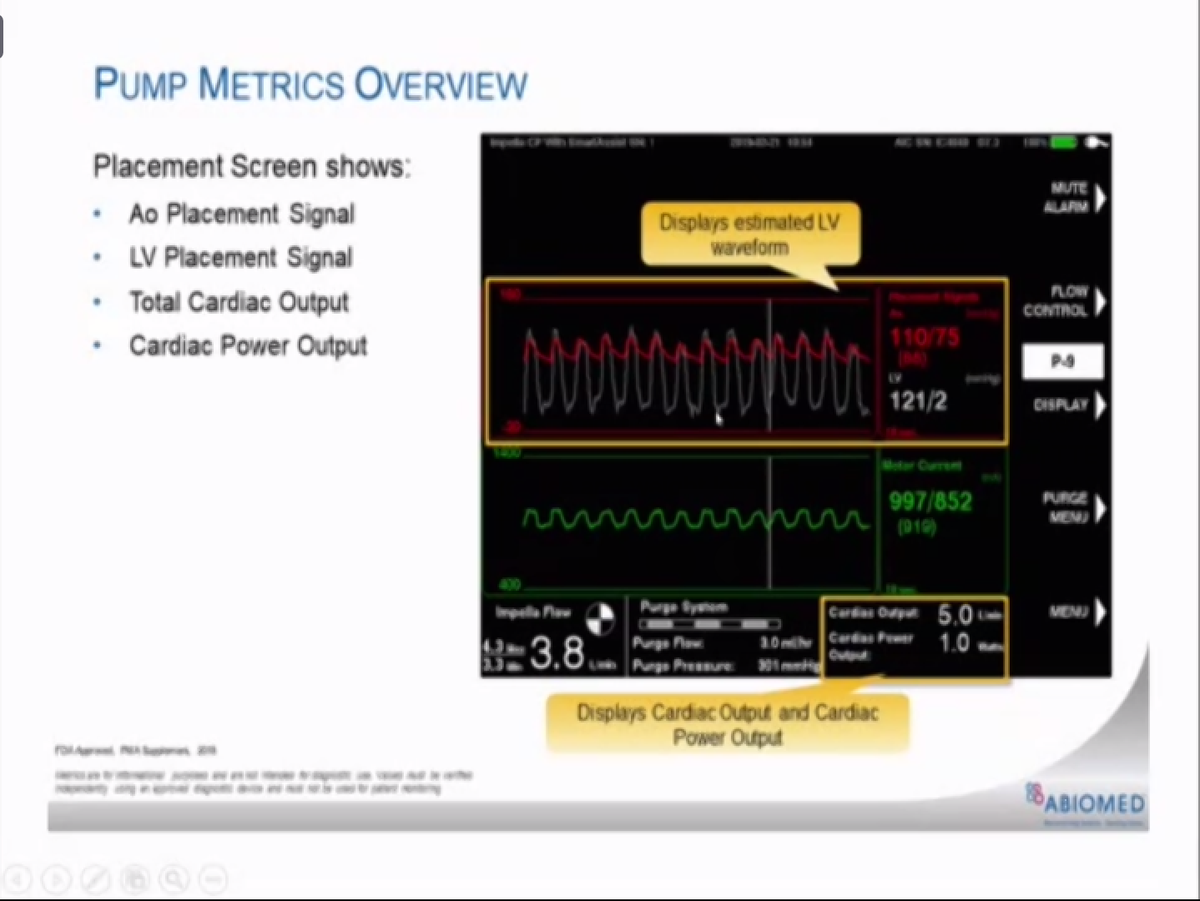
Impella
💡⬆️ MAP, afterload
💡⬇️ LVEDP
💡CO augmentation >> compared to IABP
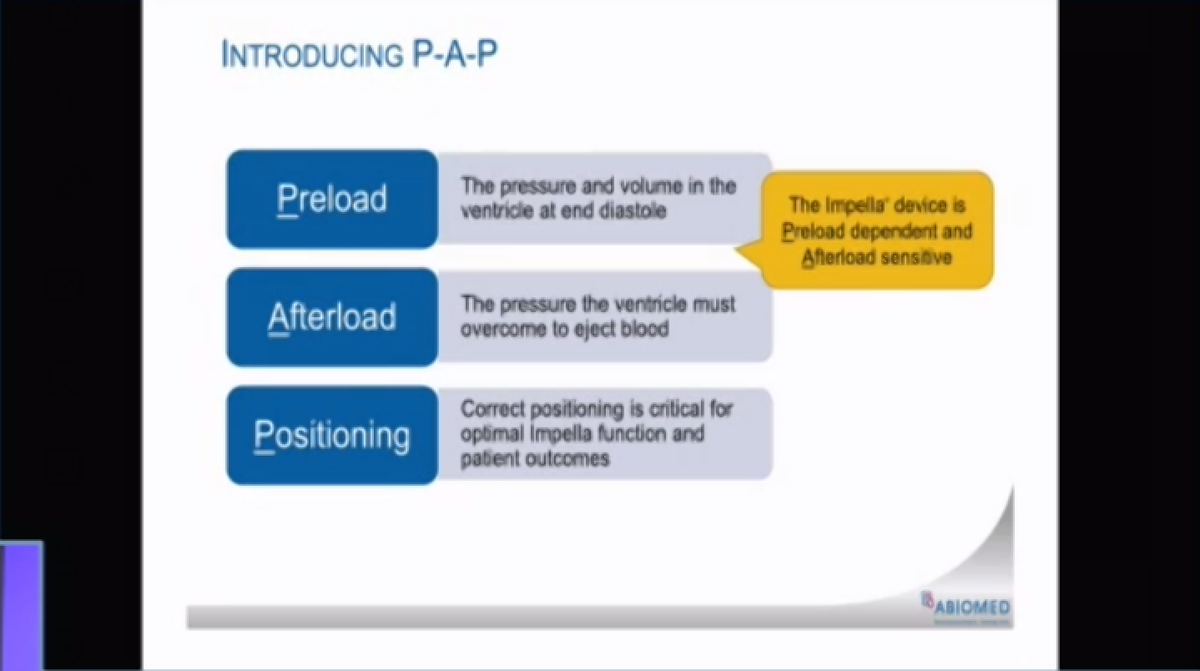
💡Pre-load dependent and afterload sensitive!
💡Position: Mid-inlet ~ 3.5 cm from AV on TTE
💡⬆️ MAP, afterload
💡⬇️ LVEDP
💡CO augmentation >> compared to IABP
💡Pre-load dependent and afterload sensitive!
💡Position: Mid-inlet ~ 3.5 cm from AV on TTE
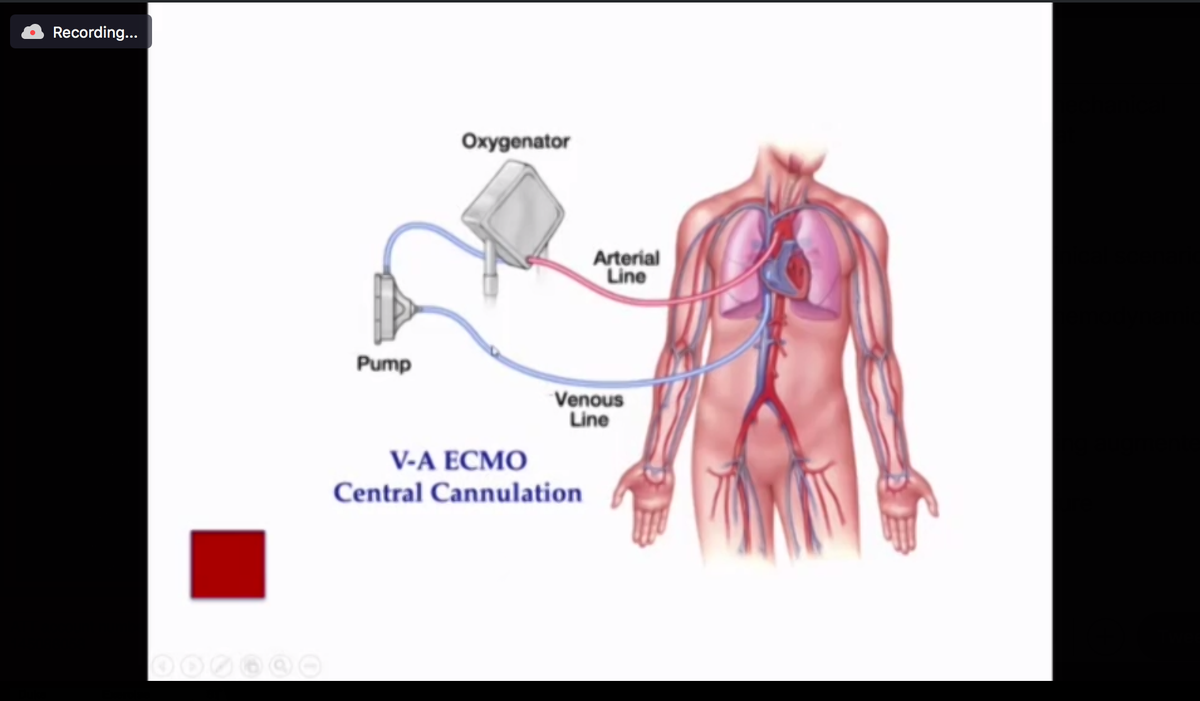
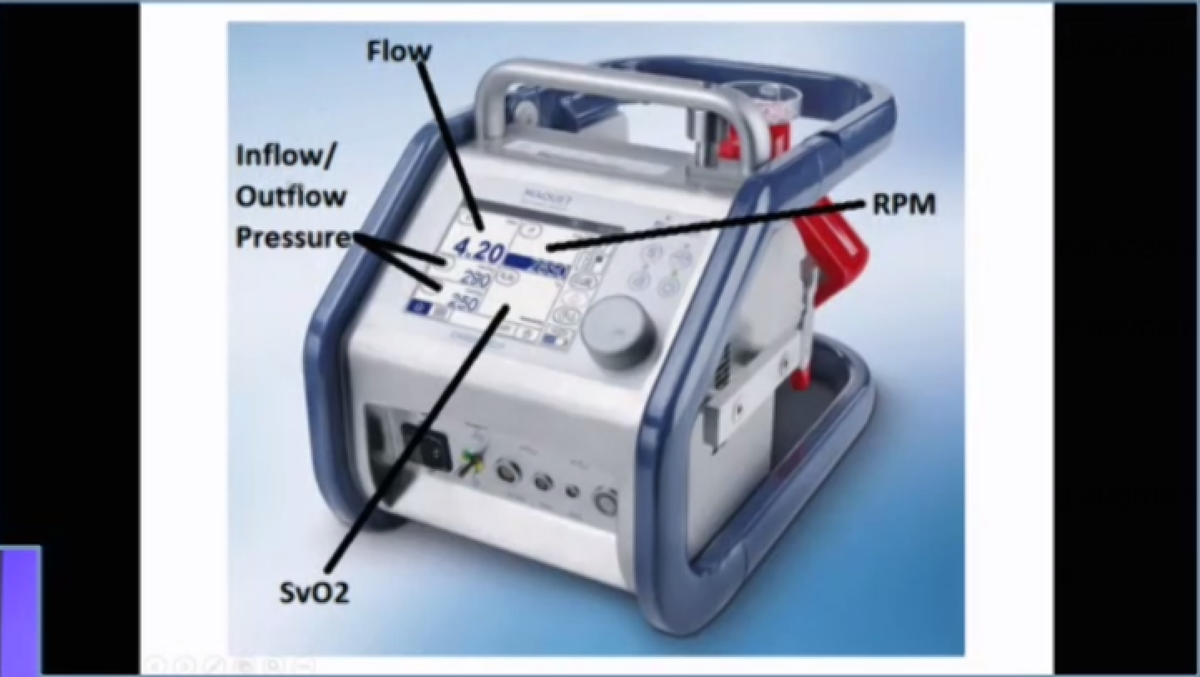
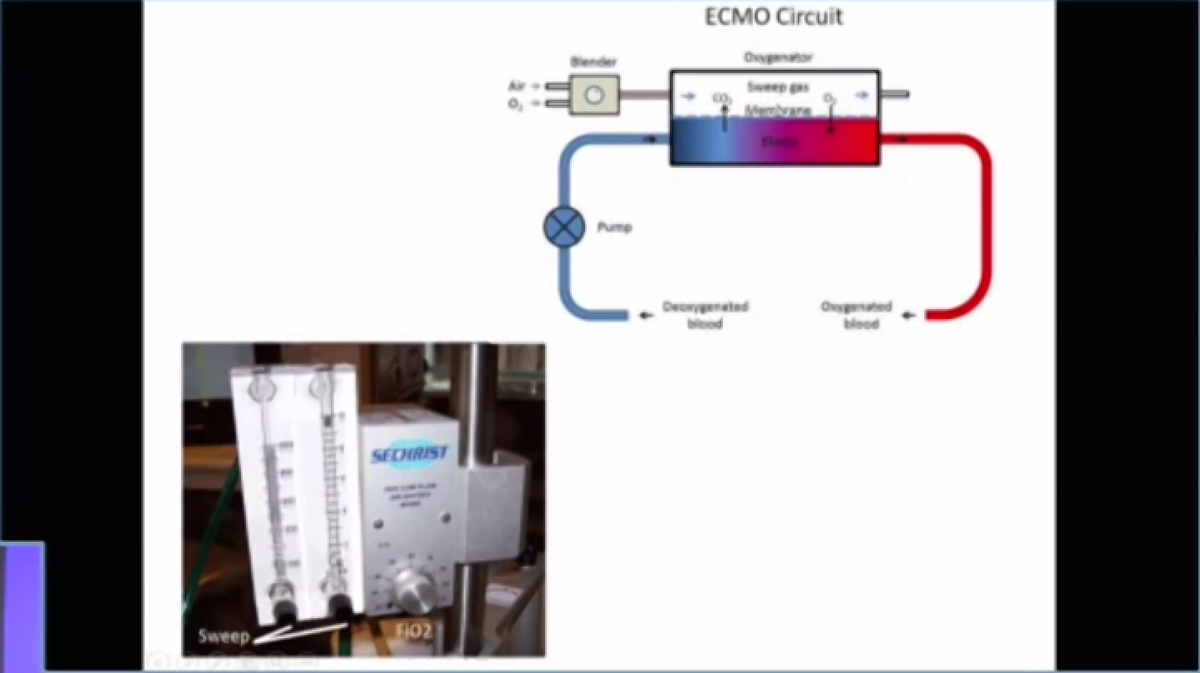
VA ECMO
💡Replaces ❤️ & 🫁
💡Adjust FiO2: ⬆️ oxygenation
💡Adjust sweep speed: ⬆️ ventilation
💡Watershed area: Where blood pumped by native ❤️ mixes with ECMO blood - matters where ABG is drawn from
💡⬆️ afterload - must ensure LV vented and AV opening to avoid catastrophe!
💡Replaces ❤️ & 🫁
💡Adjust FiO2: ⬆️ oxygenation
💡Adjust sweep speed: ⬆️ ventilation
💡Watershed area: Where blood pumped by native ❤️ mixes with ECMO blood - matters where ABG is drawn from
💡⬆️ afterload - must ensure LV vented and AV opening to avoid catastrophe!

MCS experts: If I am missing something important, please add to this in the comments!
• • •
Missing some Tweet in this thread? You can try to
force a refresh