
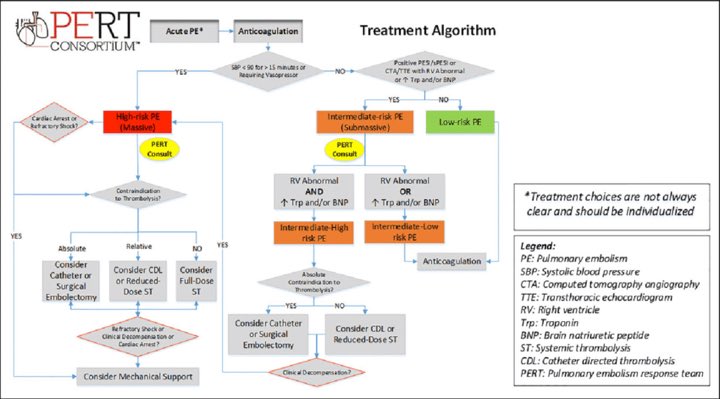
(1/22) Acute PE treatment. An ever evolving landscape.
How about a #tweetorial on acute pulmonary embolism (#PE) and how to use mechanical #thombectomy with @InariMedical #FlowTriever?? Lets goooooo!
#InariFellowsEdition #IRad #IC #cardiotwitter
Pic credit @jonathan_paulmd
How about a #tweetorial on acute pulmonary embolism (#PE) and how to use mechanical #thombectomy with @InariMedical #FlowTriever?? Lets goooooo!
#InariFellowsEdition #IRad #IC #cardiotwitter
Pic credit @jonathan_paulmd
2/ From @CDCgov data one American dies of a blood clot every....? #VTE #PE @PERTConsortium #InariFellowsForum
3/ Acute #PE stats
📊100,000–180,000 PE-related deaths annually in US
📊PE is the most preventable cause of death among hospitalized patients
📊3rd leading cardiovascular cause of death after coronary disease and stroke
⏱ 1 American dies of a blood clot every 6 seconds
📊100,000–180,000 PE-related deaths annually in US
📊PE is the most preventable cause of death among hospitalized patients
📊3rd leading cardiovascular cause of death after coronary disease and stroke
⏱ 1 American dies of a blood clot every 6 seconds

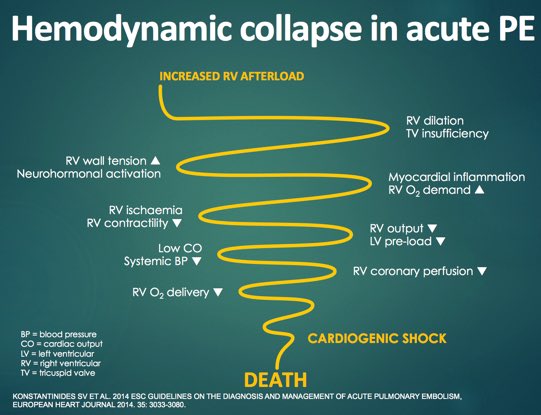
5/ For this #tweetorial we will be focusing on submassive #PE and how to treat with mechanical thrombectomy when indicated. As a #cardiologist to me its all about the patients clinical condition and the always forgotten RV! #RVstrain #InariFellowsForum
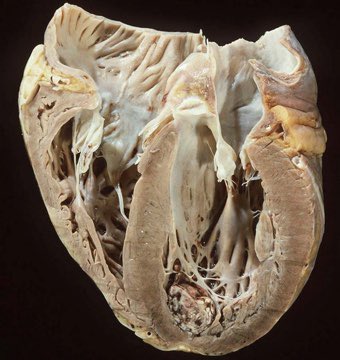
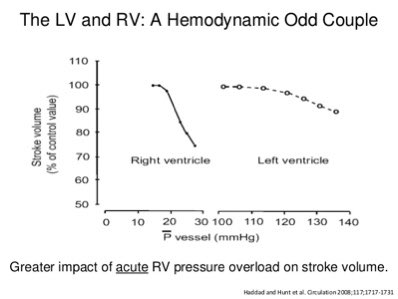
6/ The RV: Thin muscular structure that is compliant.
👍🏽GOOD at accommodating change in volume
👎🏽NOT GOOD at accommodating ACUTE changes in pulmonary pressure
#Cardiotwitter #InariFellowsForum #VTE #Hemodynamics
👍🏽GOOD at accommodating change in volume
👎🏽NOT GOOD at accommodating ACUTE changes in pulmonary pressure
#Cardiotwitter #InariFellowsForum #VTE #Hemodynamics
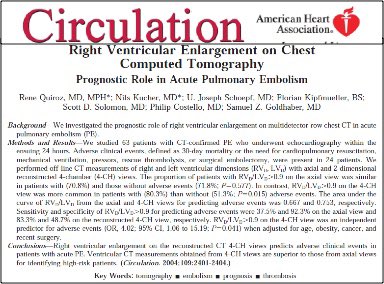
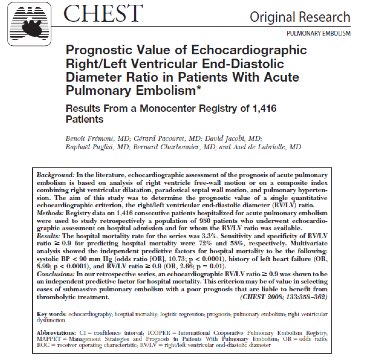
7/ People from acute PE are dying from #CARDIAC events!
Patients with RVD defined as RV/LV >0.9 have a greater chance of adverse events within 30 days. Adverse event rate at 30 days:
☠️51.3% if RV/LV ratio ≤ 0.9
☠️80.3% if RV/LV ratio > 0.9
#InariFellowsForum
Patients with RVD defined as RV/LV >0.9 have a greater chance of adverse events within 30 days. Adverse event rate at 30 days:
☠️51.3% if RV/LV ratio ≤ 0.9
☠️80.3% if RV/LV ratio > 0.9
#InariFellowsForum
8/ And since #EchoBoards are coming up don’t forget to look for McConnell’s Sign! #EchoFirst
#echo #echocardiography #cardiotwitter #VTE @ASE360 @rajdoc2005 @DocStrom @echo_stepbystep @Ivan_Echocardio @ChamsiPash @hatemsoliman @PPibarot @Miroinmi @EchoAshwag #InariFellowsForum
#echo #echocardiography #cardiotwitter #VTE @ASE360 @rajdoc2005 @DocStrom @echo_stepbystep @Ivan_Echocardio @ChamsiPash @hatemsoliman @PPibarot @Miroinmi @EchoAshwag #InariFellowsForum
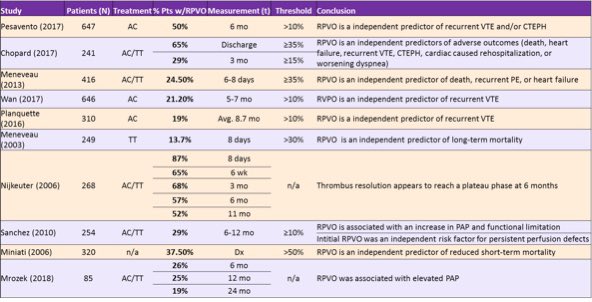
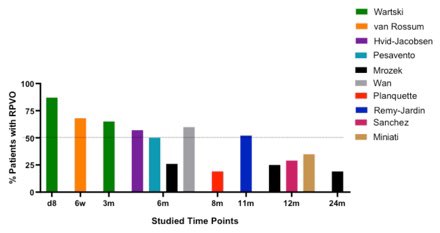
9/ Are we doing a good job with treatment? NO!
2018 MGH #PERT Data Same As 20 Years Ago! Residual thrombus ➡️poor outcomes.
90 day mortality:
☹️41.3% for massive
☹️12.3% for intermediate (ICOPER rate 20 yrs ago: 14.7%)
2/3 of intermediate-risk deaths were post discharge
2018 MGH #PERT Data Same As 20 Years Ago! Residual thrombus ➡️poor outcomes.
90 day mortality:
☹️41.3% for massive
☹️12.3% for intermediate (ICOPER rate 20 yrs ago: 14.7%)
2/3 of intermediate-risk deaths were post discharge
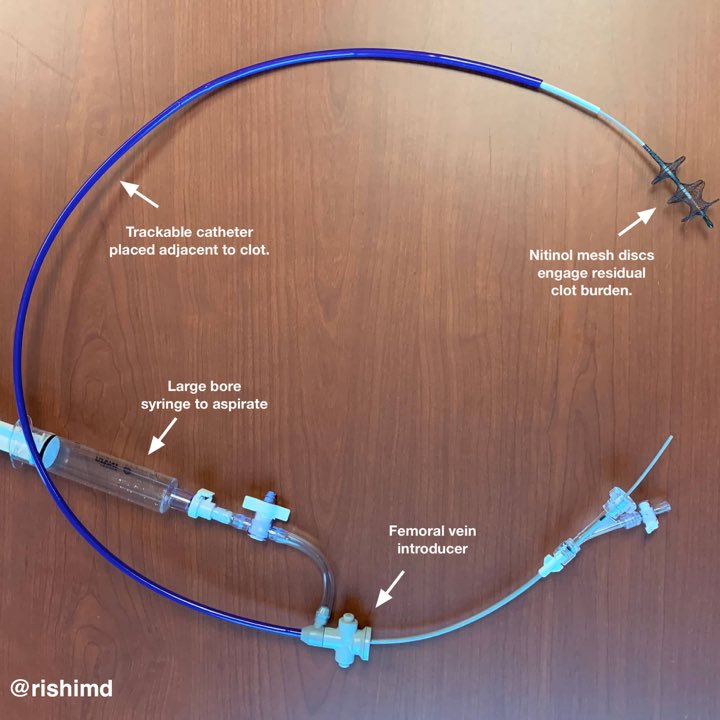
10/ So lets talk about today’s player- @InariMedical #FlowTriever
▪️FLAIR trial dem safety and ⬇️RV/LV
▪️20 F system. Powerful rapid aspiration of the clot (#Whoosh)
▪️Storage/retrieval of clot. 60 cc large bore syringe
Pic: @rishikumarmd -gotta love Cardiac Anesthesia!
▪️FLAIR trial dem safety and ⬇️RV/LV
▪️20 F system. Powerful rapid aspiration of the clot (#Whoosh)
▪️Storage/retrieval of clot. 60 cc large bore syringe
Pic: @rishikumarmd -gotta love Cardiac Anesthesia!
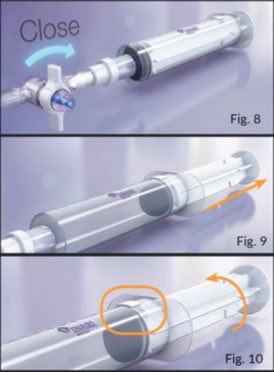
11/ An underrated and utilized aspect of this device is the ability to deploy disks to mechanically engage the clot to assist with removal.
🔑 Keys- let all them deploy and let them dwell! (Significant improvement ages 90 sec)
🔑 Crucial for removing chronic clot!
#VTE
🔑 Keys- let all them deploy and let them dwell! (Significant improvement ages 90 sec)
🔑 Crucial for removing chronic clot!
#VTE
12/ Factors favoring Mechanical #Thrombectomy
✔️Large clot burden
✔️Submassive/massive PE
✔️#Lytic ineligible/actively bleeding
✔️Need for more urgent relief
✔️Able to tolerate large venous sheath insertion
✔️Able to tolerate 1-2 hour catheter procedure
#InariFellowsForum
✔️Large clot burden
✔️Submassive/massive PE
✔️#Lytic ineligible/actively bleeding
✔️Need for more urgent relief
✔️Able to tolerate large venous sheath insertion
✔️Able to tolerate 1-2 hour catheter procedure
#InariFellowsForum
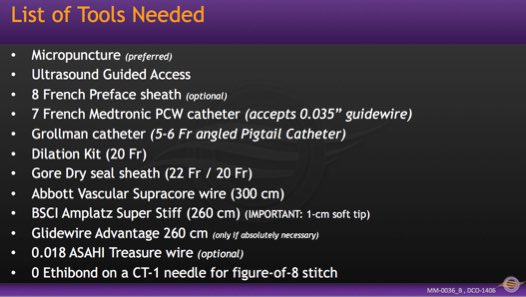
13/ List of @InariMedical tools needed! Keep this cheat sheet handy! Alright it’s #GAMETIME lets get to the steps! #InariFellowsForum #VTE
14/ STEP 1: ACCESS
💉Fem or IJ (typically femoral)
🔉Critical to use micropuncture and U/S with large bore catheter (22 Fr)
Master U/S technique. Vein usually collapses, if not use landmarks (mickey mouse view) and Doppler (vein should have continuous flow)
Be wary of prox DVT!
💉Fem or IJ (typically femoral)
🔉Critical to use micropuncture and U/S with large bore catheter (22 Fr)
Master U/S technique. Vein usually collapses, if not use landmarks (mickey mouse view) and Doppler (vein should have continuous flow)
Be wary of prox DVT!

15/ STEP 2: Crossing the tricuspid- AVOID the Chordae
🚨Special care must be taken given the size (20 Fr) of the FlowTriever System
Recommended:
🦢Swan or Baim Turi Catheter (PWP)- nice as allows 0.035 wire
▪️Alt: formed PIG
🖥Monitor hemodynamics and EKG
#InariFellowsForum
🚨Special care must be taken given the size (20 Fr) of the FlowTriever System
Recommended:
🦢Swan or Baim Turi Catheter (PWP)- nice as allows 0.035 wire
▪️Alt: formed PIG
🖥Monitor hemodynamics and EKG
#InariFellowsForum


16/ STEP 3: Wiring and Angio
🐷Exchange for PIG and take PA pressure and angio
👤If pt can hold breath, perform DSA
🗣If unable to hold, cine angiography
🔖Use images to plan landing zone of device
🔗Two strategies for wire navigation: 0.035” or 0.018”
#InariFellowsForum
🐷Exchange for PIG and take PA pressure and angio
👤If pt can hold breath, perform DSA
🗣If unable to hold, cine angiography
🔖Use images to plan landing zone of device
🔗Two strategies for wire navigation: 0.035” or 0.018”
#InariFellowsForum
17/ STEP 4: ADVANCING
👀Pay attention to your wire!
🔄Loop is good!
❌Do not advance triever without the dilator!
🖇Consider buddy wire.
🔭Consider telescope technique with T16 inside T20
#InariFellowsForum #VTR @InariMedical @HadyLichaaMD @AntoniousAttall @DrAmirKaki
👀Pay attention to your wire!
🔄Loop is good!
❌Do not advance triever without the dilator!
🖇Consider buddy wire.
🔭Consider telescope technique with T16 inside T20
#InariFellowsForum #VTR @InariMedical @HadyLichaaMD @AntoniousAttall @DrAmirKaki
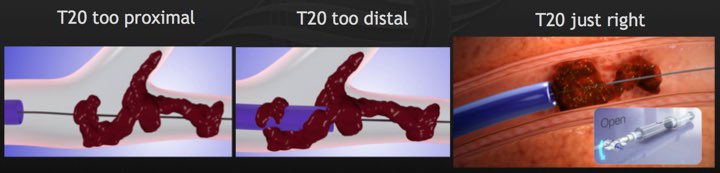
18) STEP 5: WHOOSH!
Perhaps the most important variable in max clot retrieval is: POSITION of T20 relative to the clot.
💝Optimal is 1-5 mm prox to clot for whoosh.
💞Consider “Double whoosh” if needed.
⚠️Keep wire and catheter position! ⏩Treat prox to distal.
#VTE
Perhaps the most important variable in max clot retrieval is: POSITION of T20 relative to the clot.
💝Optimal is 1-5 mm prox to clot for whoosh.
💞Consider “Double whoosh” if needed.
⚠️Keep wire and catheter position! ⏩Treat prox to distal.
#VTE
19/ STEP 6: check out the HAUL! @InariMedical @JayMathewsMD @HadyLichaaMD @DrNikkiMit @PradeepYadavMD @yuripridemd @datsunian @vcard108 @fady_iskander @t_intheleadcoat #InariFellowsForum #VTE




21/ Overall as a new IC attending and someone that admires the advancement of our field I am very excited to see what the next few years bring in regards to the tx of #VTE. There are many nuances to this procedure I couldn’t cover here but please reach out with any questions!
22/ I hope you enjoyed this #Tweetorial ! Thank you @InariMedical for putting on this free fellows course and thank you to Herman Kado and @Thomas_TuMD for sharing many of the pictures and data you’ve seen today! Have a great weekend!

