
Trying something new today - a thread on high-risk #multiplemyeloma.
I’ll focus this thread on clinical factors and will try to dive into cytogenetics/molecular biology at a later time.
This is my first "tweetorial", so any input/advice/commentary is welcome! #mmsm
1/15
I’ll focus this thread on clinical factors and will try to dive into cytogenetics/molecular biology at a later time.
This is my first "tweetorial", so any input/advice/commentary is welcome! #mmsm
1/15
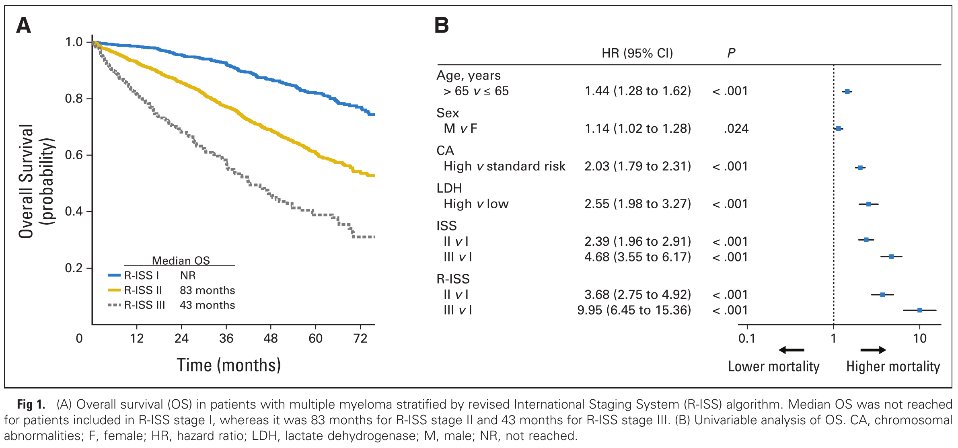
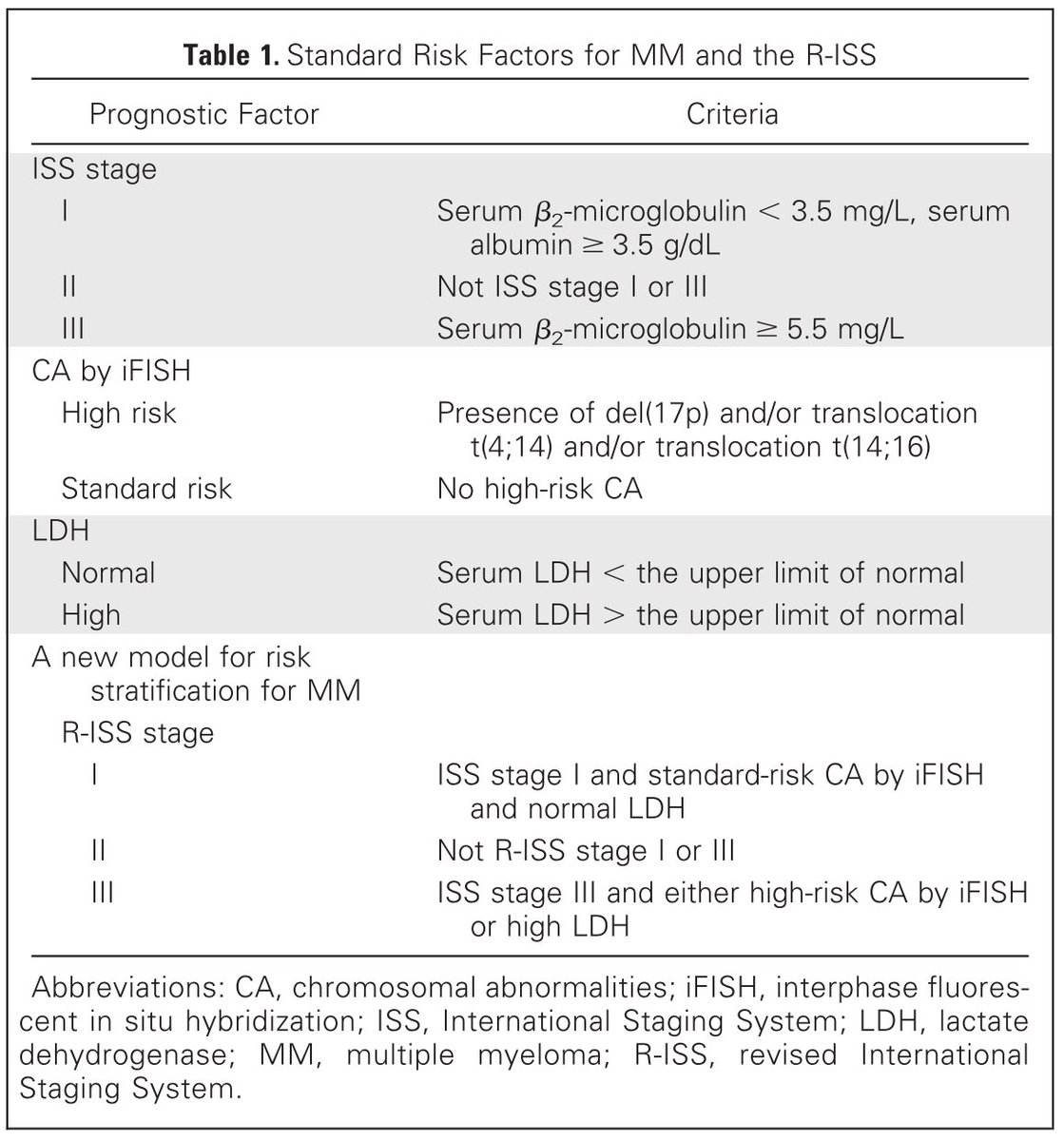
3/ The most widely used tool for risk stratification in MM today is the Revised International Staging System (R-ISS) tinyurl.com/yxjzpk5p. Pts are stratified into one of 3 “stages” based on 4 factors:
1. Albumin
2. Beta-2-microglobulin (B2M)
3. LDH
4. Cytogenetics
1. Albumin
2. Beta-2-microglobulin (B2M)
3. LDH
4. Cytogenetics
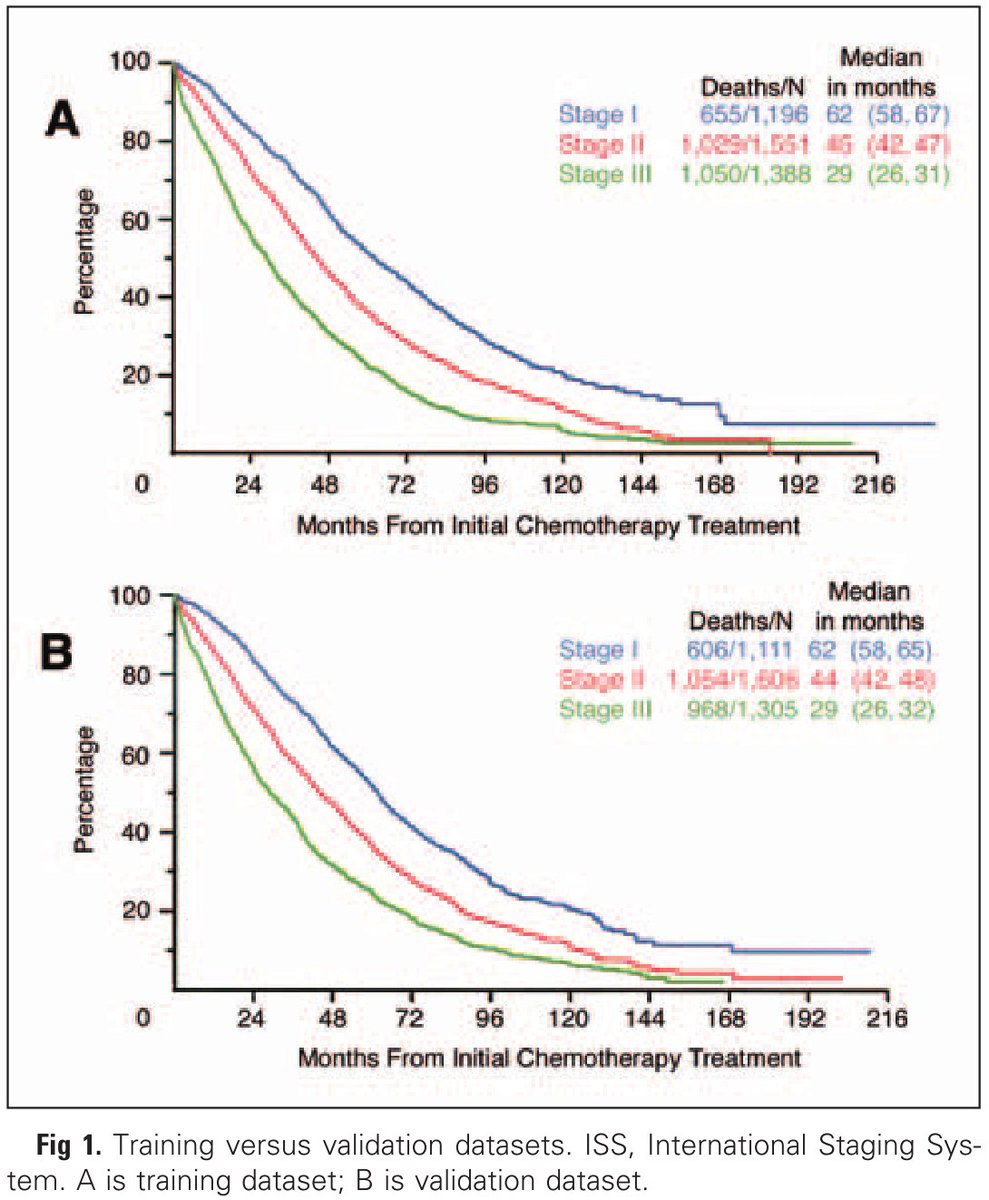
4/ Albumin and B2M were identified as key factors in the 1st ISS study. tinyurl.com/y284dvmw
These labs were found to be abnormal in many pts and this combo produced a highly reproducible risk model.
Other factors were also prognostic, but not used for various reasons.
These labs were found to be abnormal in many pts and this combo produced a highly reproducible risk model.
Other factors were also prognostic, but not used for various reasons.

5/ In MM, low albumin has been attributed to decreased hepatic synthesis due to high IL-6.
Of course, albumin levels are also be affected by other factors (i.e. nutritional status, comorbidities) that can impact survival.
Regardless, it retained significance in the chemo era.
Of course, albumin levels are also be affected by other factors (i.e. nutritional status, comorbidities) that can impact survival.
Regardless, it retained significance in the chemo era.
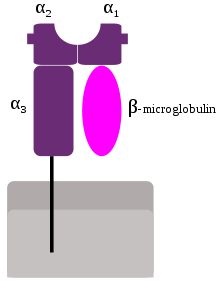
6/ B2M is a protein that is produced by all nucleated cells and associates with MHC-I.
It is highly expressed by lymphoid cells & is often⬆️in lymphoid malignancies and autoimmune conditions.
In earlier studies, high B2M was the most important prognostic factor in MM!
It is highly expressed by lymphoid cells & is often⬆️in lymphoid malignancies and autoimmune conditions.
In earlier studies, high B2M was the most important prognostic factor in MM!

7/ High B2M is mainly attributed to high tumor burden, but is also present in renal impairment (RI).
B2M is renally cleared, & plasma levels correlate with renal dysfunction. At one time it was even considered as a potential biomarker for renal function tinyurl.com/yymfvm6f
B2M is renally cleared, & plasma levels correlate with renal dysfunction. At one time it was even considered as a potential biomarker for renal function tinyurl.com/yymfvm6f
8/ Because novel MM therapies often lead to rapid improvement in RI, the negative prognostic impact of RI at dx has been significantly mitigated since publication of the ISS.
Although B2M is still used in the R-ISS, its role as a prognostic biomarker today has been questioned.
Although B2M is still used in the R-ISS, its role as a prognostic biomarker today has been questioned.
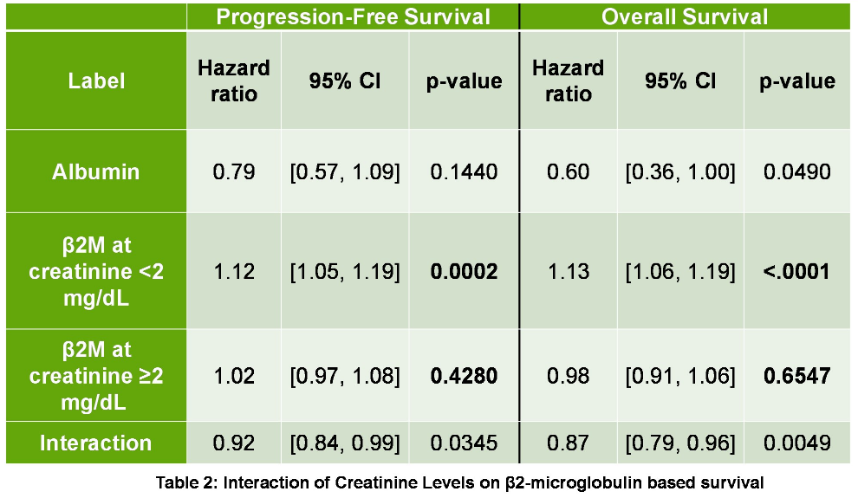
9/ The MCW group recently published that B2M was only prognostic if renal function was intact. tinyurl.com/yx8gtnzz
@rubinstein_md et al. developed a new model (MCV-SS) that replaced B2M with MCV and outperformed the R-ISS in that cohort. tinyurl.com/yy5on9a8
@rubinstein_md et al. developed a new model (MCV-SS) that replaced B2M with MCV and outperformed the R-ISS in that cohort. tinyurl.com/yy5on9a8
10/ Despite these limitations, albumin and B2M are useful baseline labs upon which MM staging is based today and should be ordered on every new and suspected MM patient.
The R-ISS has built upon the ISS by incorporating LDH and cytogenetics as prognostic factors in MM.
The R-ISS has built upon the ISS by incorporating LDH and cytogenetics as prognostic factors in MM.
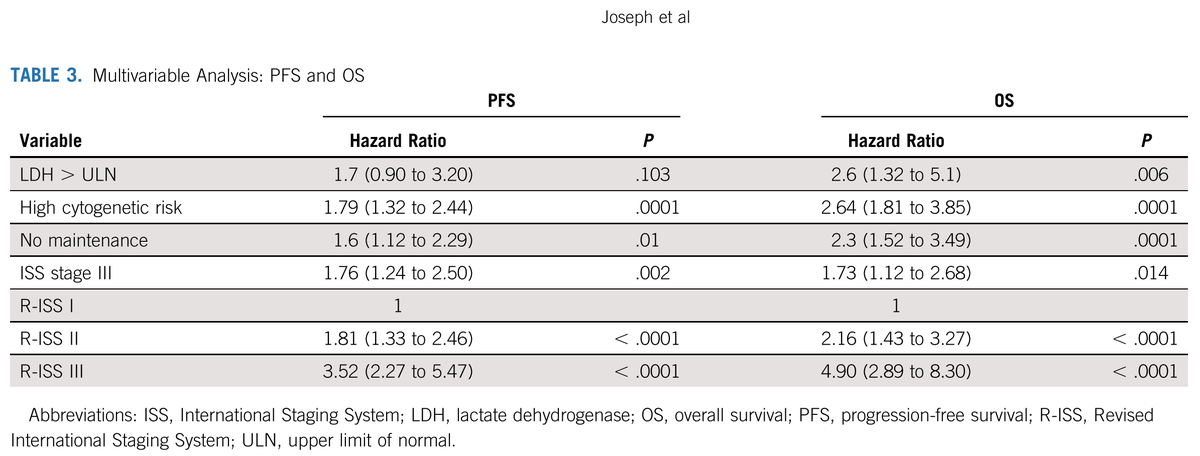
11/ LDH is notoriously nonspecific and can be elevated for many reasons, yet it is a powerful biomarker in myeloma.
Even among patients treated with current SOC regimens, LDH retains its impact, as demonstrated by the Emory group (Joseph, et al). tinyurl.com/y6foz7cu
Even among patients treated with current SOC regimens, LDH retains its impact, as demonstrated by the Emory group (Joseph, et al). tinyurl.com/y6foz7cu
12/ LDH is an intracellular enzyme that converts pyruvate to lactate during anaerobic metabolism.
LDH leaks into the bloodstream upon cell death (think ischemia, tumor lysis). In heme malignancies, this is typically due to high cell turnover, cell proliferation, active disease.
LDH leaks into the bloodstream upon cell death (think ischemia, tumor lysis). In heme malignancies, this is typically due to high cell turnover, cell proliferation, active disease.
13/ @SusanBal9 et al. evaluated the genomics of MM with high LDH in @theMMRF #CoMMpass and found⬆️cell proliferation, metastasis, and immune evasion. tinyurl.com/y5sdtj4e
Could LDH also be upregulated in the setting of BM hypoxia, which is known to⬆️VEGF, IL-6, EMD in MM?🤔
Could LDH also be upregulated in the setting of BM hypoxia, which is known to⬆️VEGF, IL-6, EMD in MM?🤔
14/ Albumin, B2M, and LDH can clearly help identify HRMM. They are altered in MM due to inflammation, proliferation, and a dysregulated bone marrow microenvironment. Often, but not always, these correspond with defined genetic aberrations & cytogenetics (separate thread to come).
15/end
It is likely that with new technologies, we will improve our understanding of the molecular biology and pathways leading to HRMM. This, coupled with risk/response-adapted treatment approaches, will hopefully help to improve outcomes for pts with HRMM. #mmsm #MedTwitter
It is likely that with new technologies, we will improve our understanding of the molecular biology and pathways leading to HRMM. This, coupled with risk/response-adapted treatment approaches, will hopefully help to improve outcomes for pts with HRMM. #mmsm #MedTwitter

