
To all who responded to our question from 8/20 a big thanks. Here is the answer and a short thread:
First the question: 15-year old with dyspnea, tachycardia, and hypotension. COVID-19 stuff is negative. Whats abnormal in the CVP tracing? Next step in definitive management is?
First the question: 15-year old with dyspnea, tachycardia, and hypotension. COVID-19 stuff is negative. Whats abnormal in the CVP tracing? Next step in definitive management is?

1) #pedsicu fellows etc. knowledge of what any normal waveform looks like is essential to tackle the abnormal. Don't worry y'all will learn more of this as you go through your fellowship training. Lots of awesome resources out there:- @OPENPediatrics learnpicu.com
2) @pccm_doc has amazing videos in @NEJM. The cincinnatichildrens.org/patients/child… app is a great resource also. I recently found grepmed.com -has phenomenal infographics
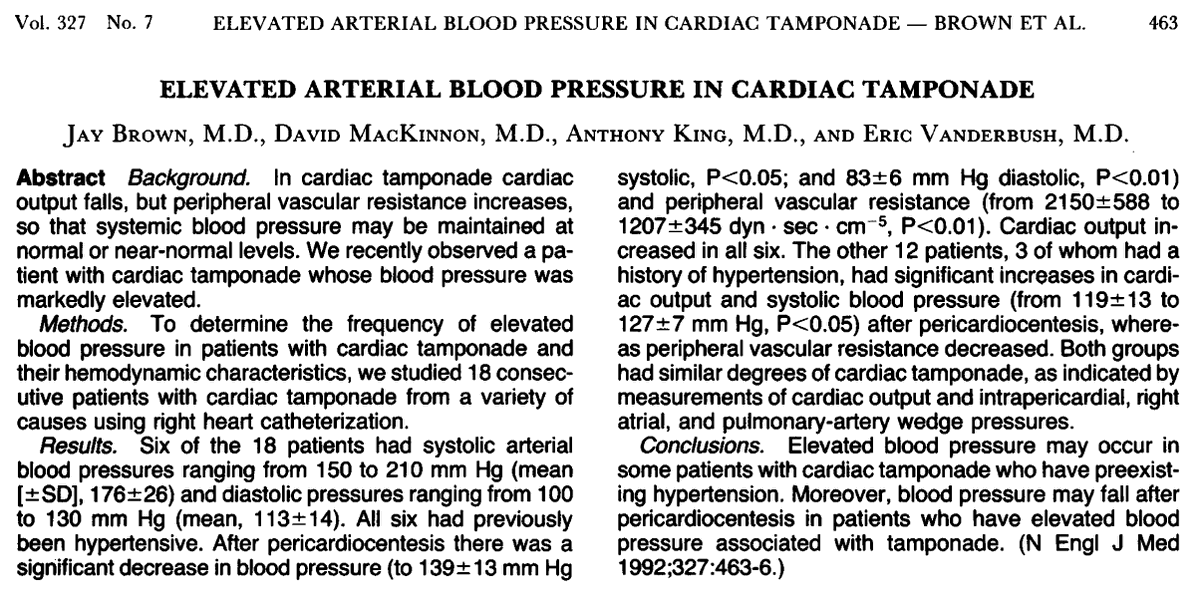
Remember just like ICP/herniation: An acute large in pericardial fluid = tamponade/collapse quickly whereas a slow large accumulation may not result in tamponade/collapse as parietal pericardium stretches +compensatory mechanisms. (Spodick D from NEJM 2003. see further below)
3)Ans: acute pericardial tamponade (PT). "blunted"(absent) Y descent is diagnostic of PT. X descent is prominent too-but thats not diagnostic of PT. Prominent X &Y descents are seen in constrictive pericarditis and restrictive cardiomyopathy. CVP will be tested on the boards.
4)Remember from @hyguruprep table:
X descent = atrial relaxation, y descent = early ventricular filling. Both are negative waveforms due to lowering of pressure.
So if pressure doesn't fall--waveform less negative (i.e blunted)
X descent = atrial relaxation, y descent = early ventricular filling. Both are negative waveforms due to lowering of pressure.
So if pressure doesn't fall--waveform less negative (i.e blunted)
5)Because early diastolic blood flow from the RA to the RV is impaired by the compressive effect of the surrounding pericardial fluid = no y descent.
X descent can be normal or dominant: Tricuspid valve is pulled away "more" (due to less bld in RV)pressure is more negative.
X descent can be normal or dominant: Tricuspid valve is pulled away "more" (due to less bld in RV)pressure is more negative.
6)Becks Triad: Hypotension, distant(muffled) heart sounds & raised JVP. Certain conditions (renal patient with severe pre-existing hypertension) may not develop hypotension with acute cardiac tamponade.
7)Pulsus paradoxus: Inspiratory systolic fall
in arterial pressure of 10 mm Hg or more during
normal breathing. Not pathognomonic of PT.
Also seen with massive PE, status asthmaticus & hemmorhagic shock.
Absence of pulsus parodoxus seen in acute pericardial tamponade is seen in
in arterial pressure of 10 mm Hg or more during
normal breathing. Not pathognomonic of PT.
Also seen with massive PE, status asthmaticus & hemmorhagic shock.
Absence of pulsus parodoxus seen in acute pericardial tamponade is seen in
8)Severe aortic regurgitation, atrial septal defects, extreme hypotension, etc.
Trivia buffs @pccm_doc may ask about Friedreich’s sign:
Deep y descent of the jugular venous waveform. Seen in constrictive pericarditis. A great video is in this link
ncbi.nlm.nih.gov/pmc/articles/P…
Trivia buffs @pccm_doc may ask about Friedreich’s sign:
Deep y descent of the jugular venous waveform. Seen in constrictive pericarditis. A great video is in this link
ncbi.nlm.nih.gov/pmc/articles/P…
9)Diagnosis of Acute pericardial Tamponade:
Echo/Pocus:
RA collapse (more specific if collapse > 30% cardiac cycle)
RV collapse (less sensitive, more specific)
Plethoric IVC. MV inflow variation >25% +effusion
EKG: Sinus tach, low QRS, electrical alternans
About alternans-
Echo/Pocus:
RA collapse (more specific if collapse > 30% cardiac cycle)
RV collapse (less sensitive, more specific)
Plethoric IVC. MV inflow variation >25% +effusion
EKG: Sinus tach, low QRS, electrical alternans
About alternans-
10)Any wave on EKG (mostly QRS) is affected. Every other QRS complex is of smaller voltage, often with reversed polarity. Large effusion can give this without tamponade. Cause: Heart is "swinging" in the fluid.
If for boards they give Cath data:
All 4 chambers = same pressures
If for boards they give Cath data:
All 4 chambers = same pressures
11)Management:
Needle paracentesis (pericardiocentesis) under echo guidance at the bedside in the PICU.
Consult cardiology/CICU attending, Avoid intubation (ketamine +fentanyl/versed for sedation), RT to hold jaw thrust/CPAP. Wouldn't make this a 1st year fellow procedure.
Needle paracentesis (pericardiocentesis) under echo guidance at the bedside in the PICU.
Consult cardiology/CICU attending, Avoid intubation (ketamine +fentanyl/versed for sedation), RT to hold jaw thrust/CPAP. Wouldn't make this a 1st year fellow procedure.
A word of caution: Posterior effusions may not be amenable to simple bedside pericardial tap. Discuss with cardiologist/Echo folks or CICU) folks. @DrBudde21 @magod_b @VForPeds @hyguruprep
12) If CPR is needed & you know patient has tamponade: CPR is ineffective unless PT drained: There is little room for additional filling & because even if systolic pressure rises, diastolic pressure falls &, in doing so, reduces coronary perfusion pressure. PALs H's & T's.
13) Great review by David Spodick @NEJM (yes from 2003 but explains stuff well)
pubmed.ncbi.nlm.nih.gov/12917306/
pubmed.ncbi.nlm.nih.gov/12917306/
14)Summary:
Pt with raised JVP, or AKI or hepatic dysfunction (transaminitis): heart evaluated (CXR, EKG, ECHO). Any Pt with dyspnea who cannot lay supine, fluid overloaded patients (pts with renal failure, nephrotics, lupus, transplant etc) deserve a cardiac eval.
@KerrynRoome
Pt with raised JVP, or AKI or hepatic dysfunction (transaminitis): heart evaluated (CXR, EKG, ECHO). Any Pt with dyspnea who cannot lay supine, fluid overloaded patients (pts with renal failure, nephrotics, lupus, transplant etc) deserve a cardiac eval.
@KerrynRoome
CVP waveforms = raison d'etre for PICU/anesthesia/cardiac fellows. Tested heavily on the boards.
Know conditions where there is no hypotension or pulsus paradoxus is absent. Not a sign of weakness to call for help (CICU/cards/RTs/other colleagues etc. prior to drainage)
Know conditions where there is no hypotension or pulsus paradoxus is absent. Not a sign of weakness to call for help (CICU/cards/RTs/other colleagues etc. prior to drainage)
Other clinicians please throw out any pearls or correct any errors I may have here.
@MKIttlesonMD @pccm_doc @GirishGDeshpan1 @FortenberryMD @hyguruprep @yoncabulutmd @agstormorken @AlexRotta #MedTwitter #AcademicTwitter @ChecchiaPaul @brownam130 @abusultaneh @JWilliamsonDO
@MKIttlesonMD @pccm_doc @GirishGDeshpan1 @FortenberryMD @hyguruprep @yoncabulutmd @agstormorken @AlexRotta #MedTwitter #AcademicTwitter @ChecchiaPaul @brownam130 @abusultaneh @JWilliamsonDO
@threadreaderapp Unroll please

