I’ve been watching with increasing concern at the trend of new daily diagnoses of COVID-19 in India over the past two weeks. To me, this reflects general public mood which seems to have begun to ignore the threat this virus poses. Thread 

While the good news is that our death rates haven’t been as bad as some of the other countries (we might debate the accuracy of death reporting), but with a population of 1.35 billion people, the absolute numbers are still sobering. And rural India is just beginning to get hit

What I’d like to see is reliable “Excess mortality” and a P score which will quantify the true impact of the pandemic on deaths in India. We know that Mumbai had an excess mortality of 13000 deaths between Apr and Jul 2020. We don’t yet have data for India as a whole.
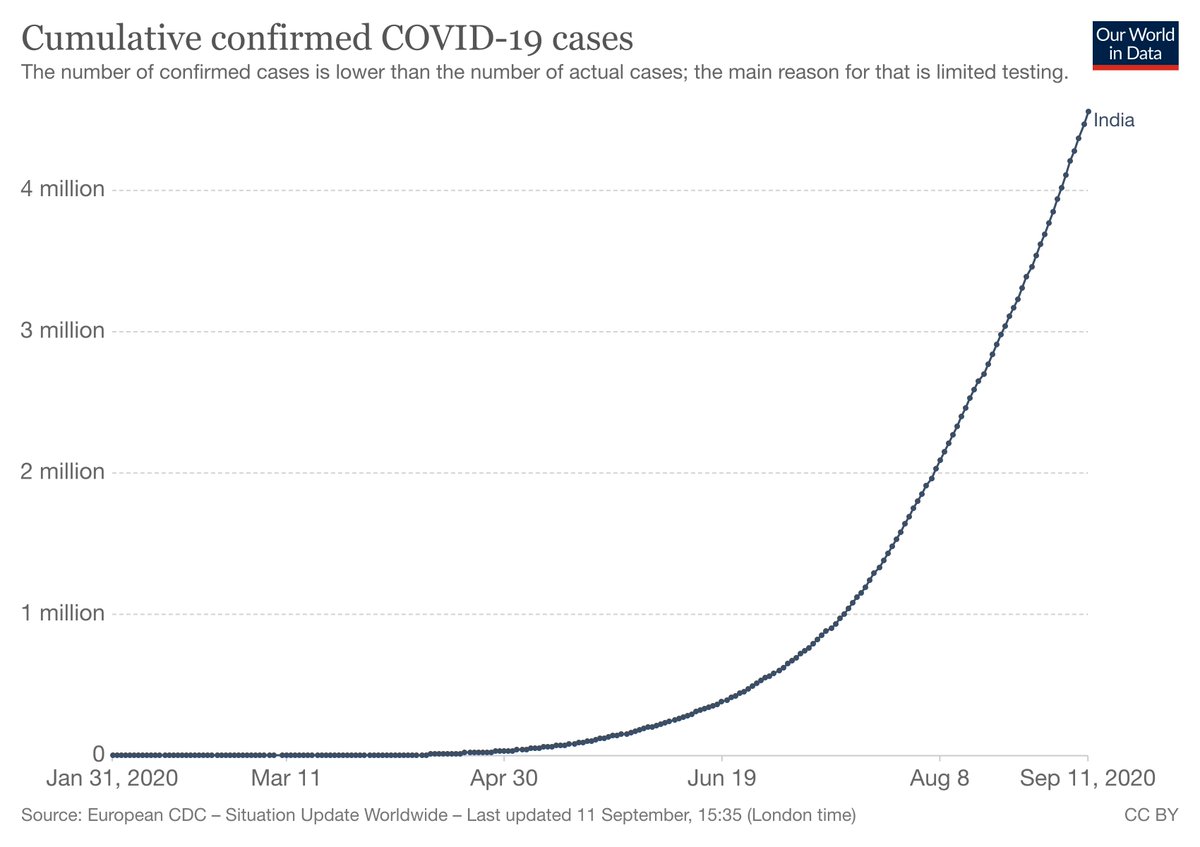
Let’s look at new daily diagnoses trends (in India) below - spaced a month apart (from today) for context
Mar 11 – 10
Apr 11 – 1035
May 11 – 4213
Jun 11 - 9996
Jul 11 – 27114
Aug 11 – 53601
Sep 11 – 96551
These are worrying numbers.
Mar 11 – 10
Apr 11 – 1035
May 11 – 4213
Jun 11 - 9996
Jul 11 – 27114
Aug 11 – 53601
Sep 11 – 96551
These are worrying numbers.
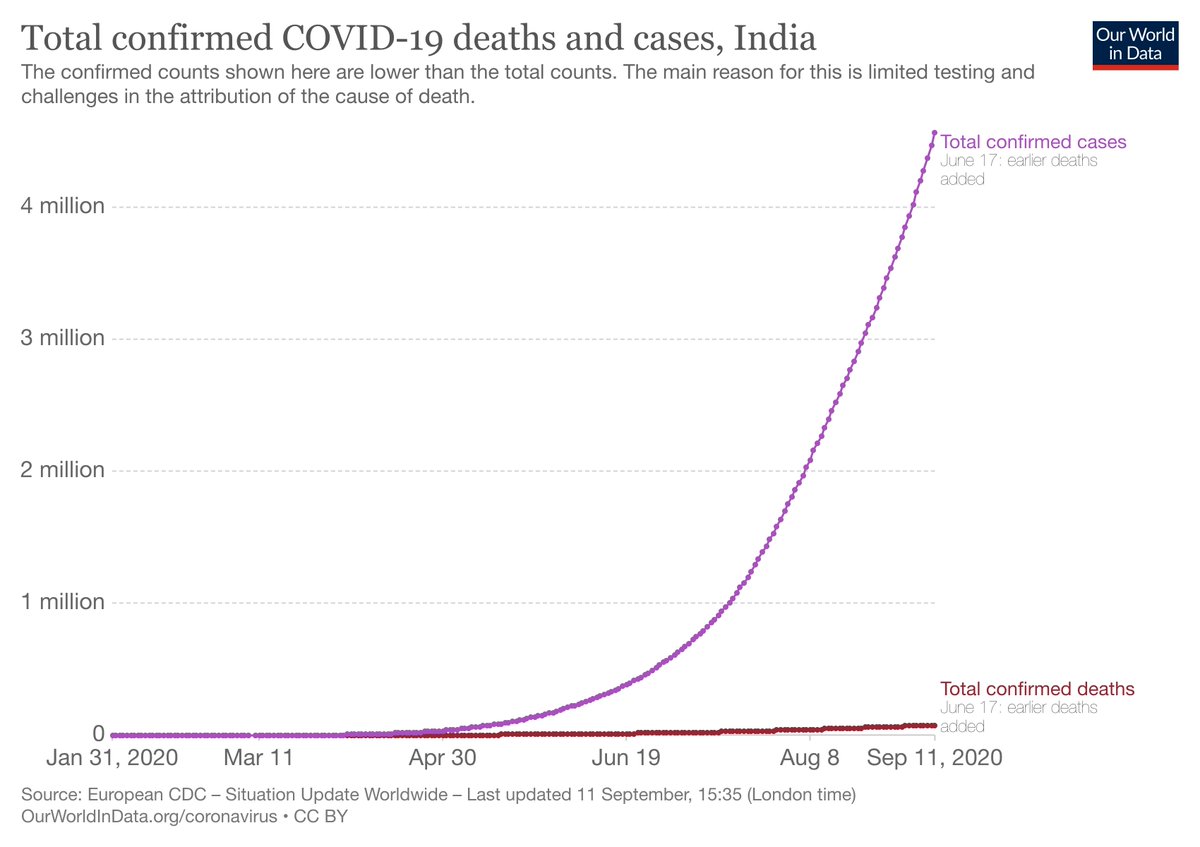
This is when (and how long we’ve taken to) cross each million (cumulative cases)
1st million – Jul 17 (168 days)
2nd – Aug 7th (20 days)
3rd – Aug 23rd (16 days)
4th – Sep 5th (13 days)
5th – Sep 16th (projected) 11 days
1st million – Jul 17 (168 days)
2nd – Aug 7th (20 days)
3rd – Aug 23rd (16 days)
4th – Sep 5th (13 days)
5th – Sep 16th (projected) 11 days
There are four known ways we can control deaths from this pandemic
1.Prevent – Masks, physical distancing & hygiene
2.Prevent - Vaccines
3.Decrease transmission – test, isolate, treat
4.Treat – Drugs, hospitalization
1.Prevent – Masks, physical distancing & hygiene
2.Prevent - Vaccines
3.Decrease transmission – test, isolate, treat
4.Treat – Drugs, hospitalization
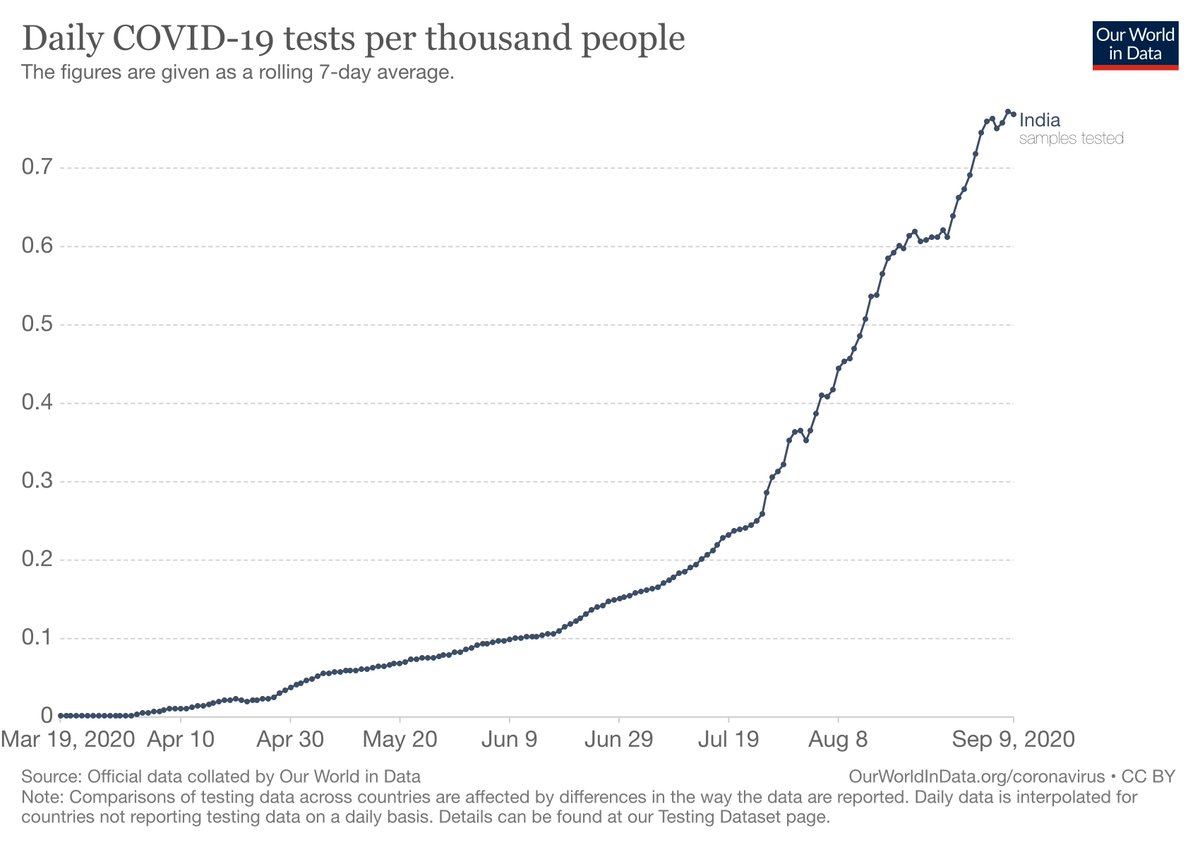
Thanks to some concerted efforts, we’ve scaled up considerably on our testing, though we could still increase availability of diagnostic testing in tier 3 cities and villages. I doubt however, that we will ever be able to do mass population testing of all asymptomatic individuals
We need to dispel myths about testing too – popular belief is that anyone who has come in contact with a confirmed #COVID_19 patient needs immediate testing.
Fact: what high risk contacts really need is quarantine, with testing between day 5 and 14 of exposure
Fact: what high risk contacts really need is quarantine, with testing between day 5 and 14 of exposure
We could certainly try and ramp up our treatment facilities, and rationalize hospitalization. Triaging the need for hospital admission, oxygen beds and ICU care makes sense when the infrastructure is inadequate. Lesson for the future though is urgent reform of healthcare systems
#COVID_19 has been a wake-up call for improving healthcare in India. Our investment in public healthcare facilities needs to at least double in the next 2 years; quadruple in 5 years. Linking quality to government hospitals is key, making them the go-to for the common man/woman
Treatment strategies (in spite of the thousands of trials) have been fairly disappointing for #COVID_19. With the exception of steroids (decreased mortality) and to a lesser extent Remdesivir (faster clearance), there have been no dramatic proven therapies
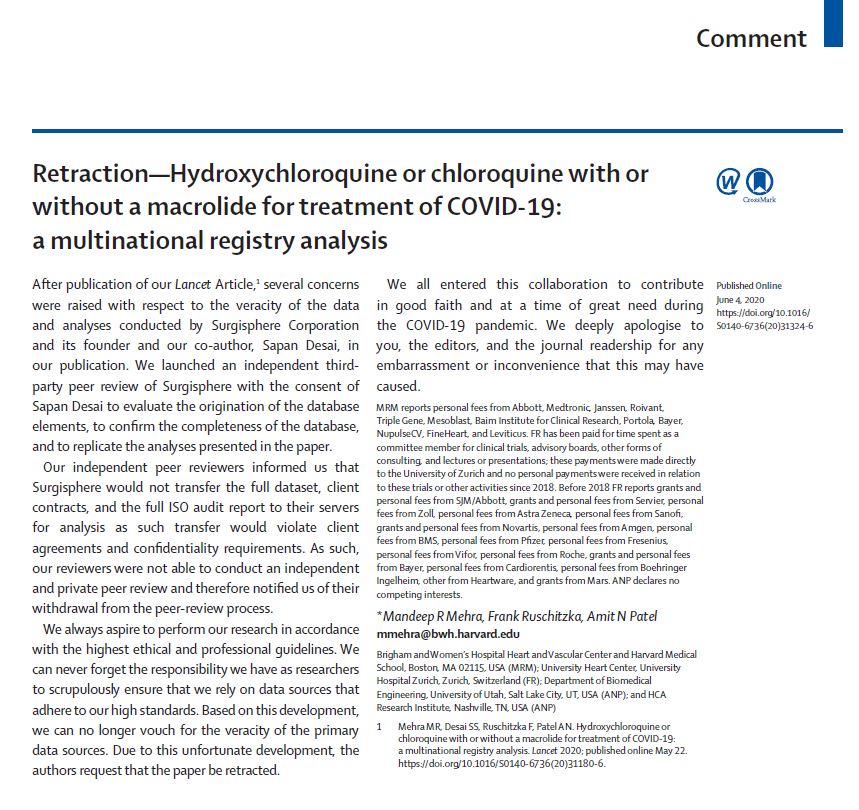
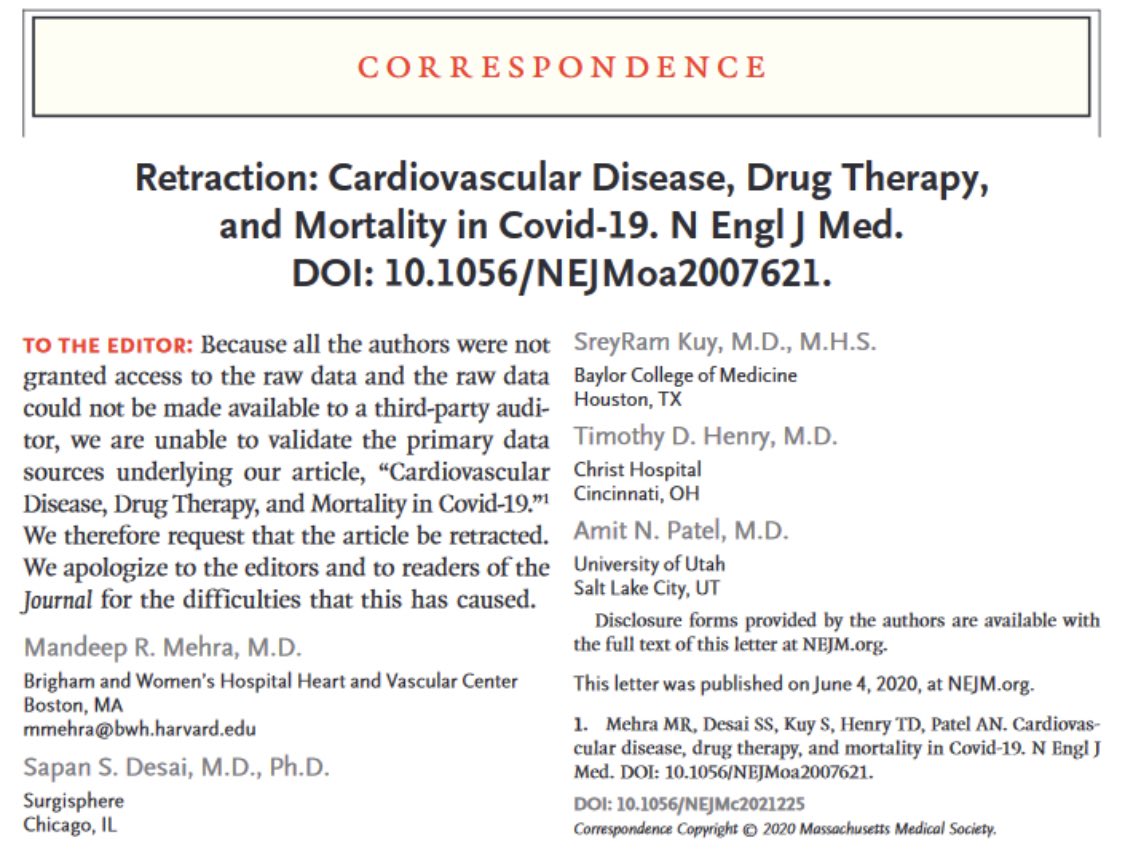
#COVID_19 has also taught us not to jump the gun with “promising” therapies. From #HCQ to #ConvalescentPlasma to other drugs (monoclonals, other antivirals), all of which were touted as “proven” treatment options, only to be debunked by randomized trials
When you look at the 100s of 1000s of patients treated by these drugs, I can’t help thinking of what a wasted opportunity it’s been. UK prioritized #RECOVERY as one large pragmatic trial where all patients would be enrolled, & see what they’ve achieved! @PeterHorby @MartinLandray
What we need to do in India is to make sure we don’t get carried away with unproven claims and allow the desperation of the pandemic to “do something” and use ineffective drugs to treat. That is just a wasteful use of resources when we already have significant constraints
Which brings us to prevention as a strategy to control the pandemic. Clearly the best option now (and has always been). There are 160+ vaccine candidates, and 26 in human trials. Vaccines are great, but they are not a panacea, for various reasons
First, vaccines need to be proven safe & effective before being used at population level. This takes time. Second, even after it’s proven to be effective, it takes time to manufacture enough to cover the world’s population. And make it available at a cost countries can afford
Finally, we’re not really sure how effective the vaccine will be. We all hope that it will provide effective immunity to protect from subsequent infection, but we can’t base our entire strategy on that. Which then leaves us with…
Basic precautionary measures – not glamorous, not high tech, yet likely the only thing we can bank on to reduce transmission, and finally control the pandemic. The three Ws – Wear masks, Watch your distance, and Wash your hands
Strangely, and paradoxically as the pandemic has progressed, we seem to have de-emphasized our messaging on following these simple, yet effective measures
When we had 1000 new diagnoses/day, we were extremely careful, didn’t step out of our homes, wore masks when in public, maintained physical distancing and washed our hands frequently. Ironically, with close to 100,000 new diagnoses a day, we’ve thrown caution to the winds
People seem to have equated the government lifting lockdowns to the virus not being a problem anymore. Nothing can be further from the truth as the numbers above show. We need to de-link the two.
We need to get our messaging right now – we’re seeing the highest number of cases, the highest number of daily deaths than ever before in this pandemic. Now is the most dangerous phase we've had during the pandemic so far, and this is no time to let our guard down.
While lifting the lockdown was (and is) necessary, adherence to basic precautionary measures are crucial. We just cannot afford to ignore this. We need to widely disseminate the need for the three Ws – Wear a mask, Watch your distance, Wash your hands
• • •
Missing some Tweet in this thread? You can try to
force a refresh