#ASEchoJC #Tweetorial on #WASE
World
Alliance
Societies of Echocardiography
Normal Values Study
#Echofirst most widely used imaging modality BUT
WHAT IS NORMAL for ❤️ size & function?
bit.ly/32pKxAC @JournalASEcho
World
Alliance
Societies of Echocardiography
Normal Values Study
#Echofirst most widely used imaging modality BUT
WHAT IS NORMAL for ❤️ size & function?
bit.ly/32pKxAC @JournalASEcho
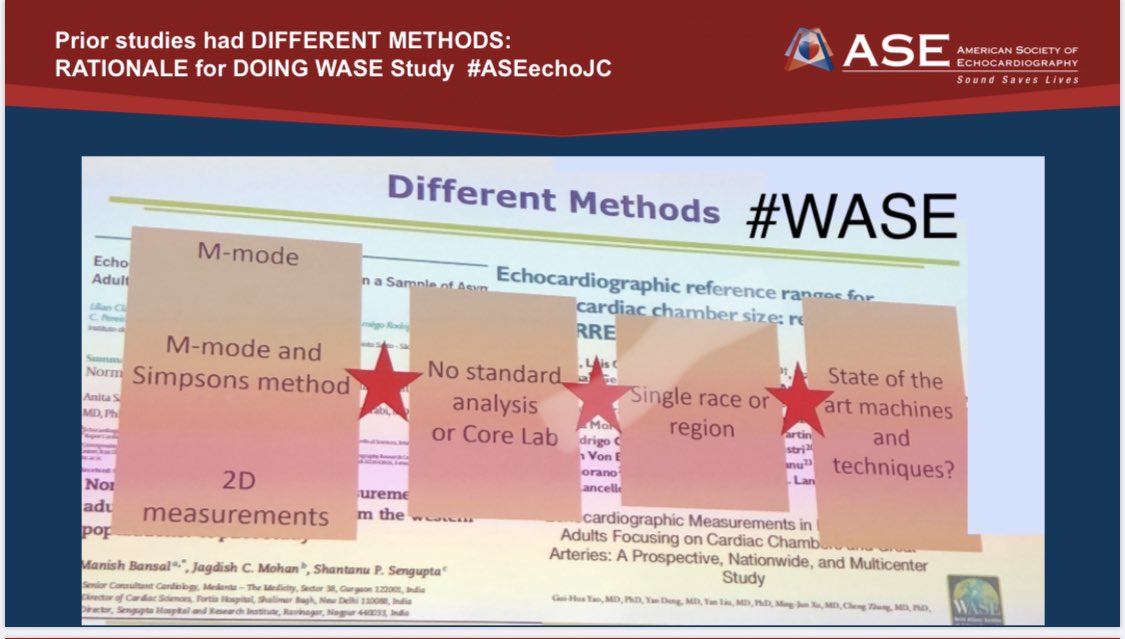
2/ Prior ❤️measurement studies:
❤️used VARIOUS methods- M mode, M mode & simpsons, 2D
❤️No standard analysis or core lab
❤️Only single race or country/region
❤️?? State of the art machines or techniques
❤️Need for a prospective international observational study #WASE was born
❤️used VARIOUS methods- M mode, M mode & simpsons, 2D
❤️No standard analysis or core lab
❤️Only single race or country/region
❤️?? State of the art machines or techniques
❤️Need for a prospective international observational study #WASE was born
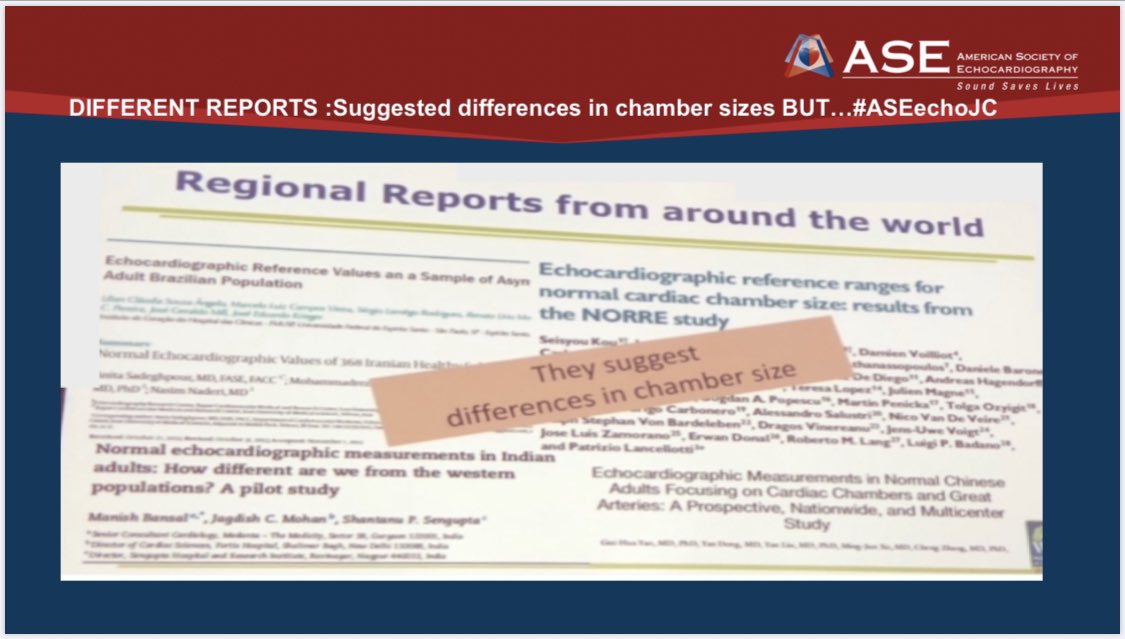
3/#DiversityandInclusion
@ASE360 @escardio #EACVI recommended normal values used all over the 🌎 but only represent normal Caucasian people from USA & Europe
bit.ly/3irijv5 #ASEchoJC
@ASE360 @escardio #EACVI recommended normal values used all over the 🌎 but only represent normal Caucasian people from USA & Europe
bit.ly/3irijv5 #ASEchoJC

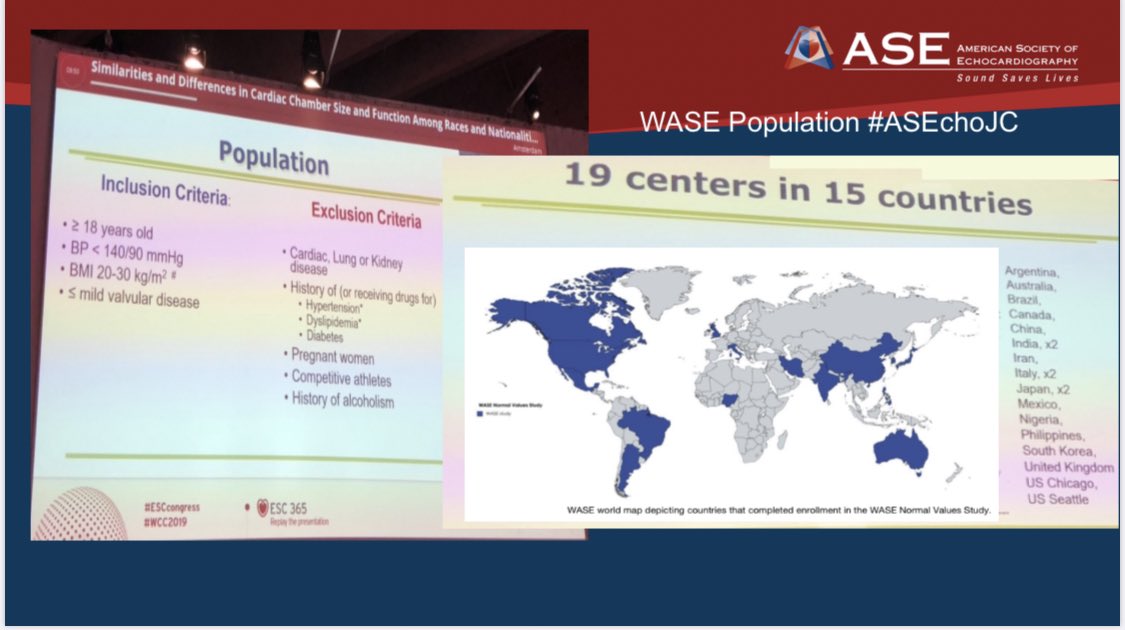
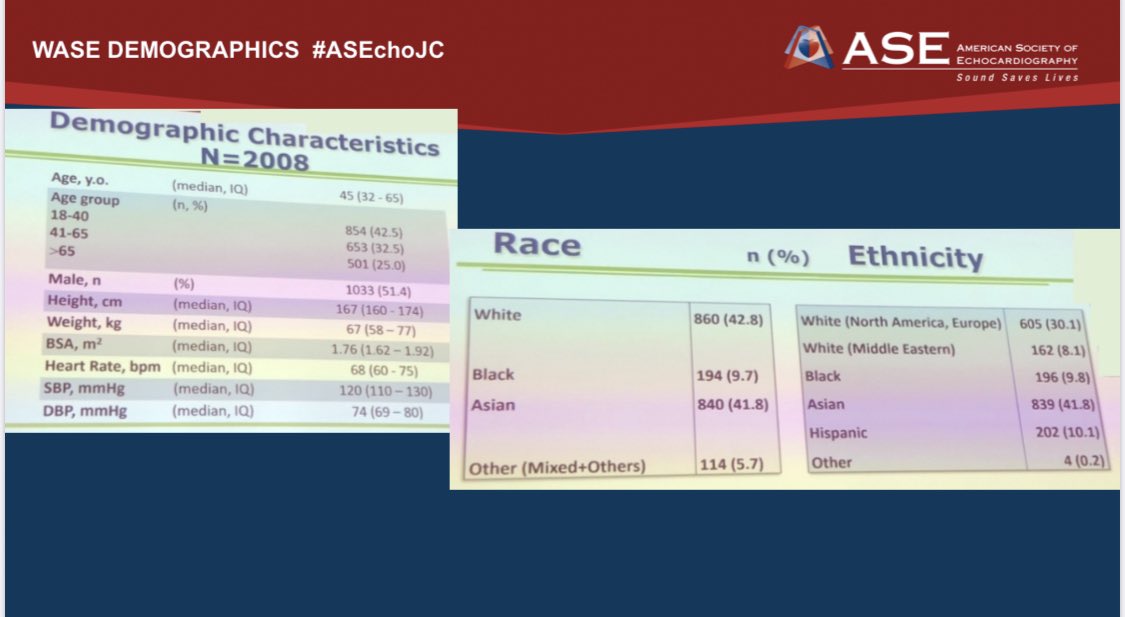
4/#PopulationHealth studied
❤️>2000 people from 15 countries
❤️similar age distribution in all countries
❤️dif races/ethnicities 🌎
❤️Excluded: pregnancy
Competitive athletes, diseases: No DM or HTN or Kidney,lung,or known ❤️ Dz #ASEchoJC #WASE @dr_benoy_n_shah
❤️>2000 people from 15 countries
❤️similar age distribution in all countries
❤️dif races/ethnicities 🌎
❤️Excluded: pregnancy
Competitive athletes, diseases: No DM or HTN or Kidney,lung,or known ❤️ Dz #ASEchoJC #WASE @dr_benoy_n_shah

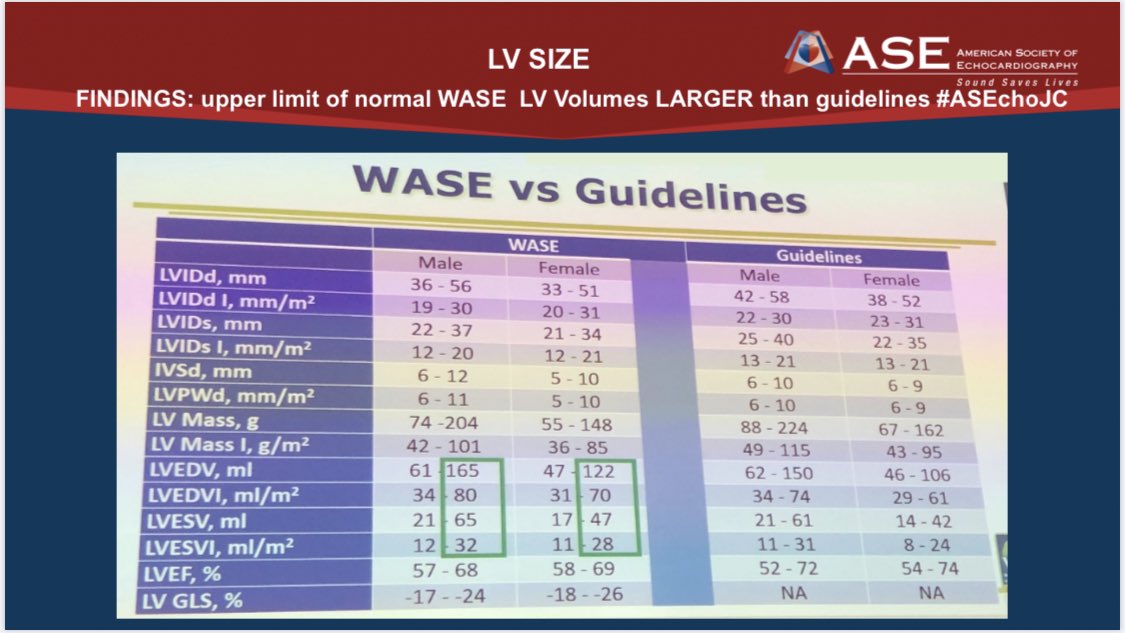
5/LV size & function measured LV linear dimensions, volumes, mass, EF,GLS @TOMTEC_IMAGING #echofirst #ASEchoJC

6/Findings:
LV dimensions & volumes are larger in males, while LVEF and GLS are higher in females. #ASEchoJC #Echofirst
LV dimensions & volumes are larger in males, while LVEF and GLS are higher in females. #ASEchoJC #Echofirst


7/ Findings:
Heart size by LVEDVi is same for blacks and whites but smaller for Asians (in fact largest difference b/w ♥️ is Indian and Australia in both sexes) #ASEchoJC
Heart size by LVEDVi is same for blacks and whites but smaller for Asians (in fact largest difference b/w ♥️ is Indian and Australia in both sexes) #ASEchoJC

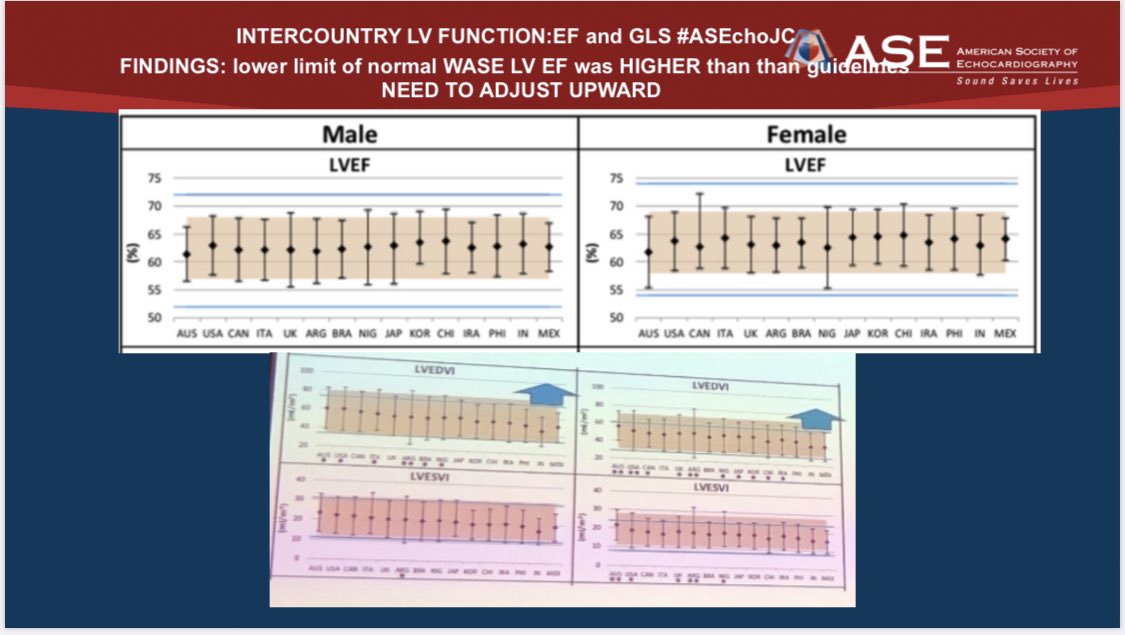
9/Findings: Lower limit of Normal WASE EF was HIGHER than guidelines #ASechoJC : need to adjust lower cutoff of “normal ” upward in guidelines
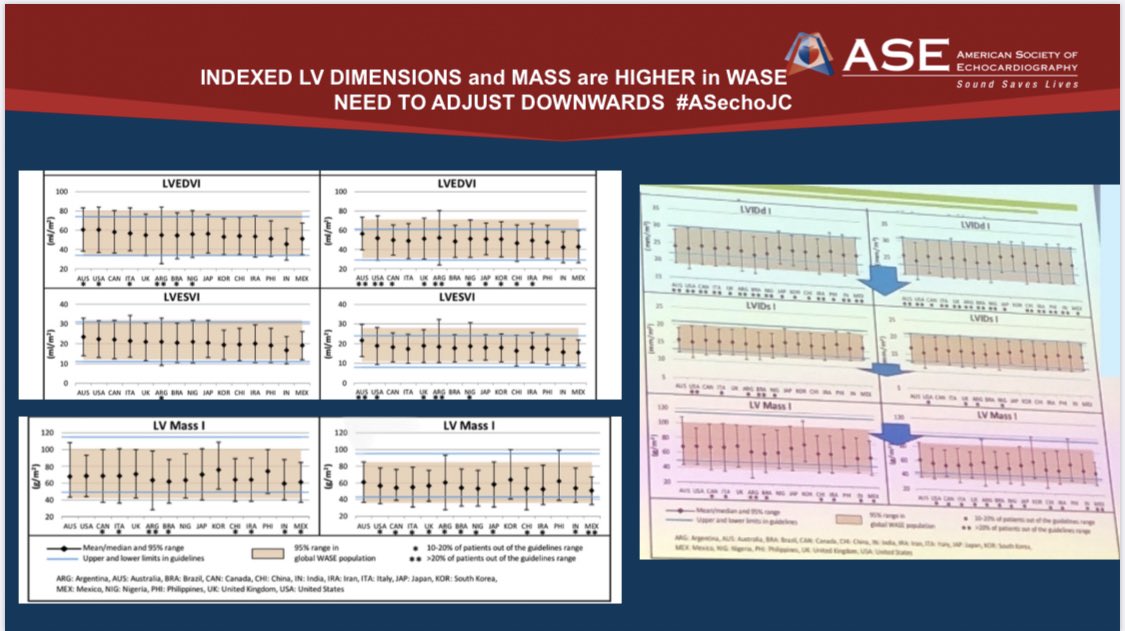
10/“normal” Indexed LV dimensions(size) & Mass are higher in #WASE & guidelines should adjust downwards
#ASEchoJC
Join us Tuesday 9/15 night 8 pm for the discussion
#ASEchoJC
Join us Tuesday 9/15 night 8 pm for the discussion
• • •
Missing some Tweet in this thread? You can try to
force a refresh