We may be systematically underestimating R by excluding students in halls of residence. A Thread
We know that data on the Government Coronavirus dashboard is unreliable (see this thread)
https://twitter.com/Dr_D_Robertson/status/1312865098843779083
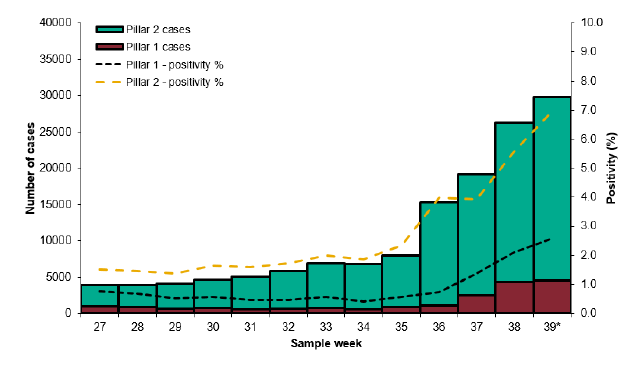
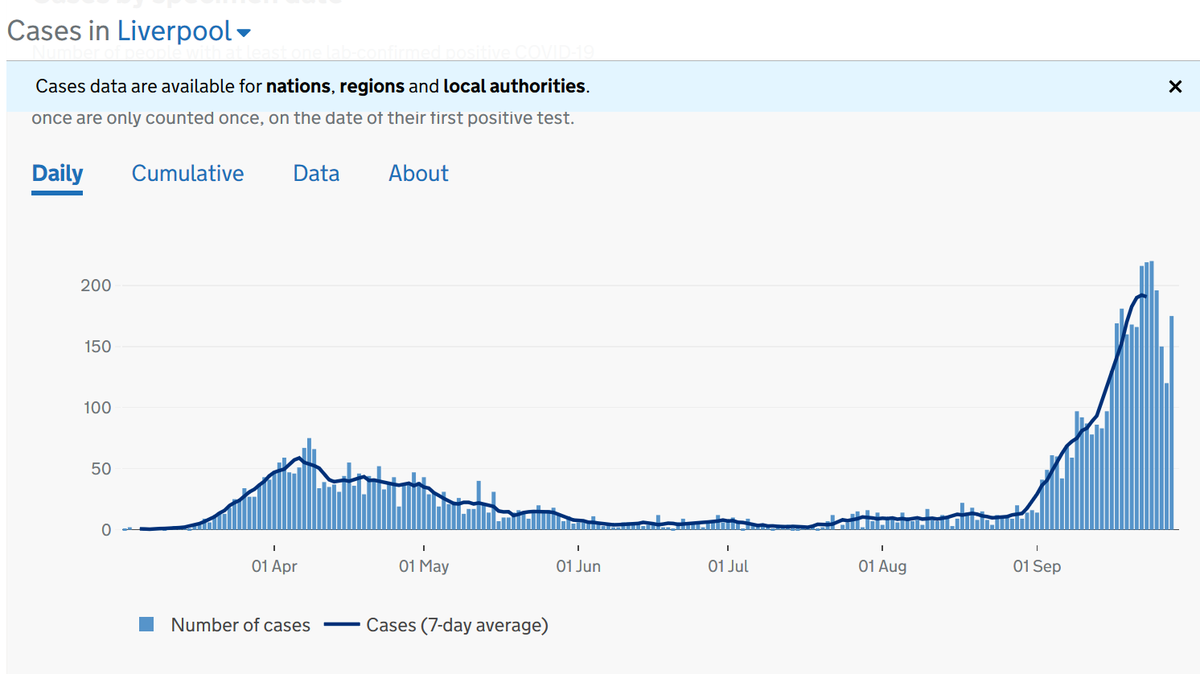
We also know that we are not doing enough testing as the positivity rate is so high (7% overall for Pillar 2 tests and up to 15% in some areas such as Liverpool) (see this thread)
https://twitter.com/Dr_D_Robertson/status/1312821471618662401
So, how do we go about estimating R? Here's a thread I wrote in January explaining R in relation to Covid-19 (which then didn't have an official name) duncanrobertson.com/2020/01/24/con…
To estimate R, we carry out surveys - which means you pick a representative group of people, either households or individuals, and test them repeatedly.
There are two main surveys: ONS and REACT
There are two main surveys: ONS and REACT
ONS excludes student halls of residence, as 'only private residential households, otherwise known as the target population in this bulletin, are included in the sample. People in hospitals, care homes and other institutional settings are not included'
ons.gov.uk/peoplepopulati…
ons.gov.uk/peoplepopulati…

This is confirmed here sciencemediacentre.org/expert-reactio…

The REACT survey uses GP lists to generate its sample of people who are tested.
But of course, new students are only just registering with their GPs, and it is unclear when the GP lists were pulled for the latest study (Round 5 of REACT-1, 18-26 Sep)
imperial.ac.uk/media/imperial…
But of course, new students are only just registering with their GPs, and it is unclear when the GP lists were pulled for the latest study (Round 5 of REACT-1, 18-26 Sep)
imperial.ac.uk/media/imperial…

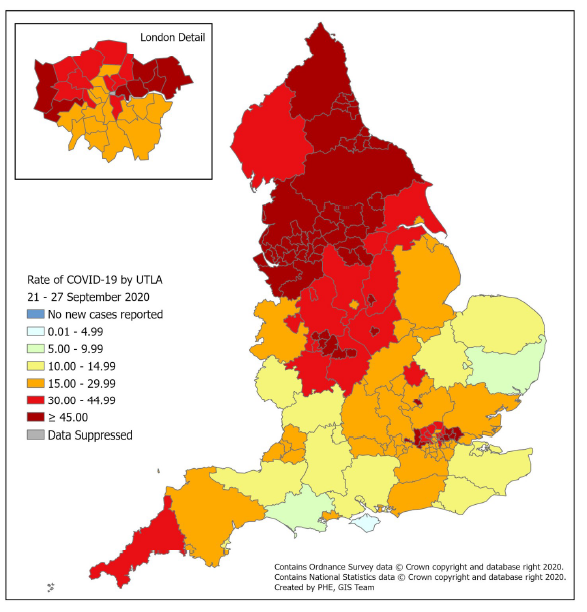
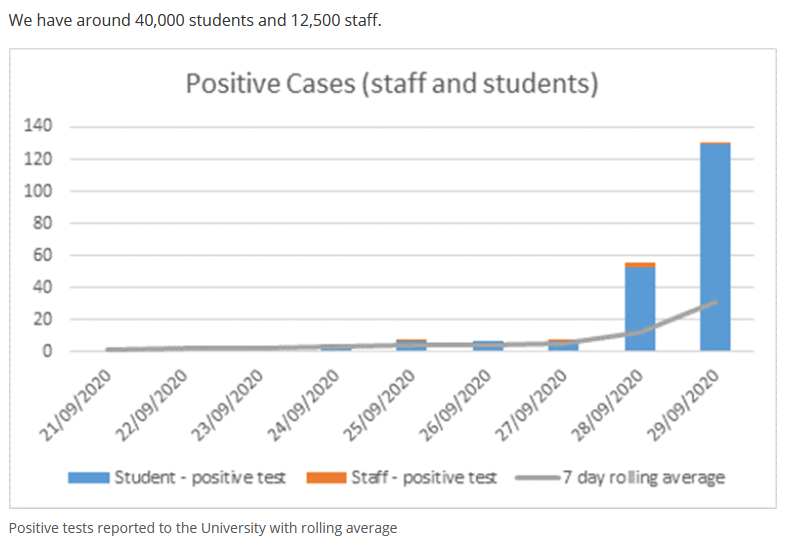
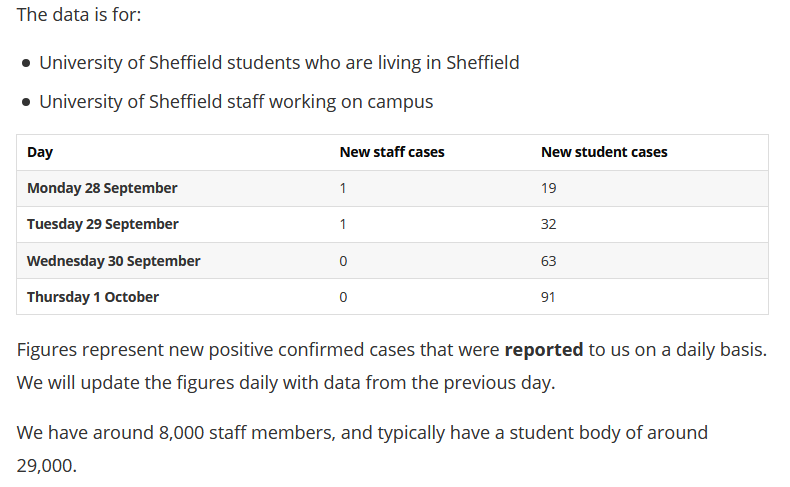
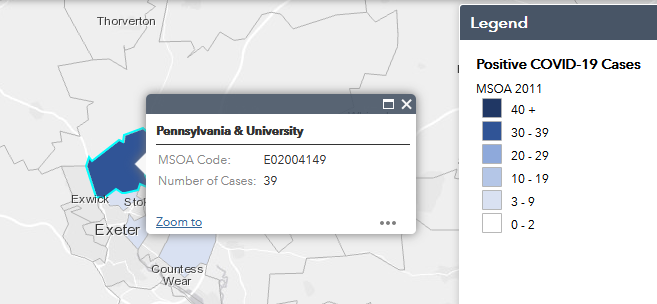
We know that halls of residence are a significant driver of transmission.
We may be systematically under-sampling from halls of residence and therefore systematically underestimating R.
We may be systematically under-sampling from halls of residence and therefore systematically underestimating R.
• • •
Missing some Tweet in this thread? You can try to
force a refresh