COVID-19: An EBM Take Part 2 at #ACOEP20
-Anticoagulation
-Awake Proning
-Invasive Mechanical Ventilation
-ECMO
-Hydroxychloroquine
#FOAMed #FOAMcc @ACOEP
-Anticoagulation
-Awake Proning
-Invasive Mechanical Ventilation
-ECMO
-Hydroxychloroquine
#FOAMed #FOAMcc @ACOEP

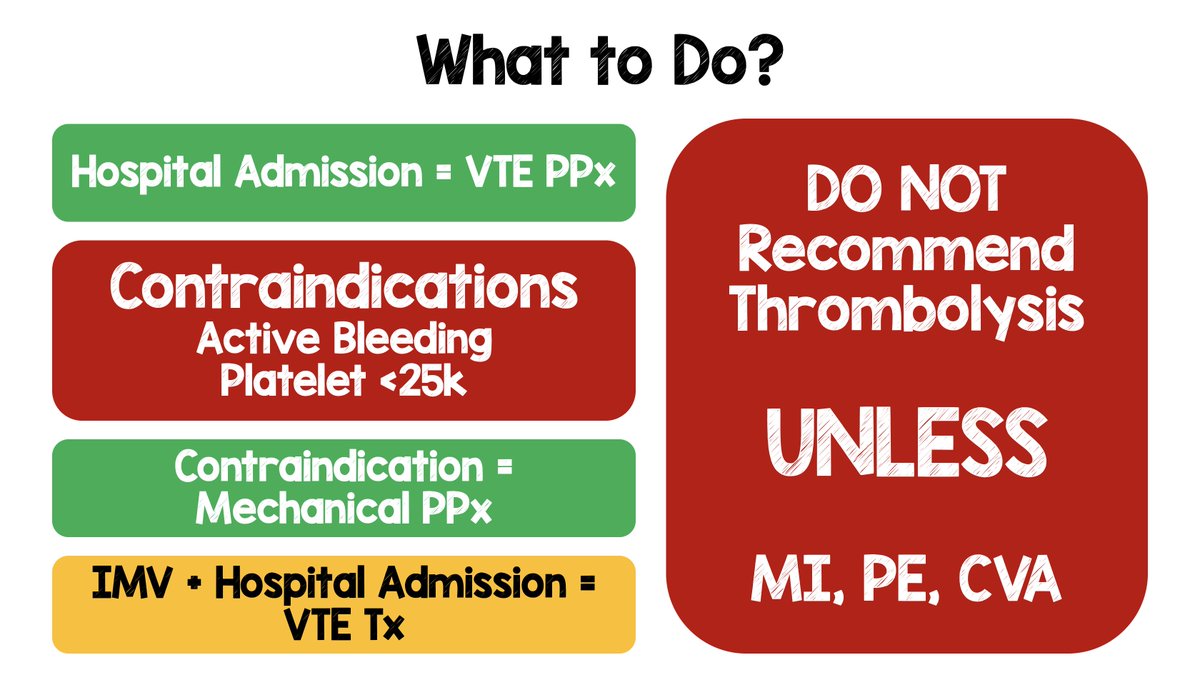
Anticoagulation in #COVID19
-Admitted pts = weight based prophylaxis (unless contraindications)
-IMV = therapeutic anticoagulation
-Intermediate dosing has ZERO evidence base
-Thrombolysis --> Only if other indication (i.e. MI, PE, CVA)
#FOAMed #FOAMcc @ACOEP
-Admitted pts = weight based prophylaxis (unless contraindications)
-IMV = therapeutic anticoagulation
-Intermediate dosing has ZERO evidence base
-Thrombolysis --> Only if other indication (i.e. MI, PE, CVA)
#FOAMed #FOAMcc @ACOEP

Awake Proning in #COVID19
-Will not work on everyone
-Longer duration is better than shorter duration
-Pts require frequent assessments as they can become prone and O2 dependent (DO NOT ADMIT to Regular Floor)
#FOAMed #FOAMcc @ACOEP
-Will not work on everyone
-Longer duration is better than shorter duration
-Pts require frequent assessments as they can become prone and O2 dependent (DO NOT ADMIT to Regular Floor)
#FOAMed #FOAMcc @ACOEP

Invasive Mechanical Ventilation in #COVID19
-Early disease is high compliance disease
-Try to delay intubation with HFNC or NIV
-High compliance = PEEP ≤15cmH20 + Higher FiO2 (Don't follow ARDSnet as can cause harm)
-Tolerate lower O2 sats (88 to 94%)
#FOAMed #FOAMcc @ACOEP
-Early disease is high compliance disease
-Try to delay intubation with HFNC or NIV
-High compliance = PEEP ≤15cmH20 + Higher FiO2 (Don't follow ARDSnet as can cause harm)
-Tolerate lower O2 sats (88 to 94%)
#FOAMed #FOAMcc @ACOEP

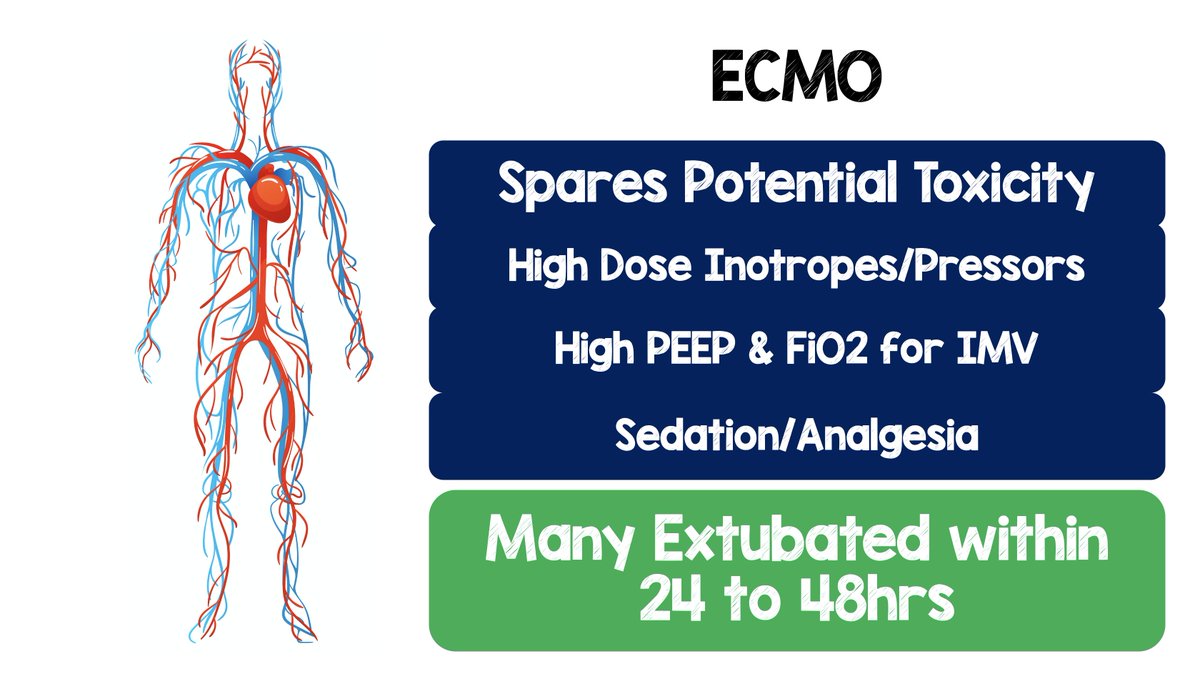
ECMO in #COVID19
-ECMO as salvage therapy can be a bridge to nowhere
-ECMO earlier in disease spares potential toxicities of high dose pressors, High PEEP, High FiO2, & sedation/analgesia
-May pts extubated within 24 to 48hrs
-Pt selection is key in order for this to work
-ECMO as salvage therapy can be a bridge to nowhere
-ECMO earlier in disease spares potential toxicities of high dose pressors, High PEEP, High FiO2, & sedation/analgesia
-May pts extubated within 24 to 48hrs
-Pt selection is key in order for this to work

Hydroxychloroquine in #COVID19
-Early data showed reduced viral load
-Subsequent data showed no effect on mortality or prophylaxis
-Potential increase in cardiac dysrhythmias
-Evidence DOES NOT support use of HCQ
#FOAMed #FOAMcc @ACOEP
-Early data showed reduced viral load
-Subsequent data showed no effect on mortality or prophylaxis
-Potential increase in cardiac dysrhythmias
-Evidence DOES NOT support use of HCQ
#FOAMed #FOAMcc @ACOEP
• • •
Missing some Tweet in this thread? You can try to
force a refresh