Local contact tracing is where local authorities set up local teams to contact cases that the national team is unable to reach within 24hrs.
They're seen as part of the solution to rising case numbers in England.
They're seen as part of the solution to rising case numbers in England.
And with good reason. Early data from places like Blackburn with Darwen @BWDDPH suggest that they're able to reach up to 9 out of 10 cases that couldn't be contacted by the national team.
manchestereveningnews.co.uk/news/uk-news/h…
manchestereveningnews.co.uk/news/uk-news/h…
Some of the cases that that national team miss don't want to be reached and won't ever engage.
Some just missed the call or didn't recognise the number.
And others are likely to be more vulnerable, socially isolated, digitally deprived, transient, or economically worse off.
Some just missed the call or didn't recognise the number.
And others are likely to be more vulnerable, socially isolated, digitally deprived, transient, or economically worse off.
So simple things like having a local phone number and a local voice seem to work. Plus speaking the right language, being able to visit people at home, and provide support to help with isolation.
Essentially, knowing the local population and how to reach vulnerable groups.
Essentially, knowing the local population and how to reach vulnerable groups.
The idea of local contact tracing's generally been well received.
LAs are keen to get local systems set up to help with rising cases. And it's a partnership - it helps T&T, and the national T&T/PHE support the local authorities to get going with advice/templates etc.
LAs are keen to get local systems set up to help with rising cases. And it's a partnership - it helps T&T, and the national T&T/PHE support the local authorities to get going with advice/templates etc.
Initially national support was prioritised for areas with most need.
The @lgcplus report that 73 upper tier authorities will be live by mid-month - that's about half.
lgcplus.com/politics/coron…
The @lgcplus report that 73 upper tier authorities will be live by mid-month - that's about half.
lgcplus.com/politics/coron…
Models will vary. Some will be 5 day services, some 7 day. Some include knocking on doors, others just call handlers.
And the variation is entirely driven by local resources to staff the systems, the capacity and time available to get them up and running.
And the variation is entirely driven by local resources to staff the systems, the capacity and time available to get them up and running.
They take a massive effort to get off the ground - colleagues across legal, ICT, customer services, environmental health, comms, public health, information gov, community services, finance, and more.
And everyone's already busy up to their eyeballs.
And everyone's already busy up to their eyeballs.
But it's an additional tool for local authorities trying to cope. And that's appealing.
However, it's getting harder for LAs to manage.
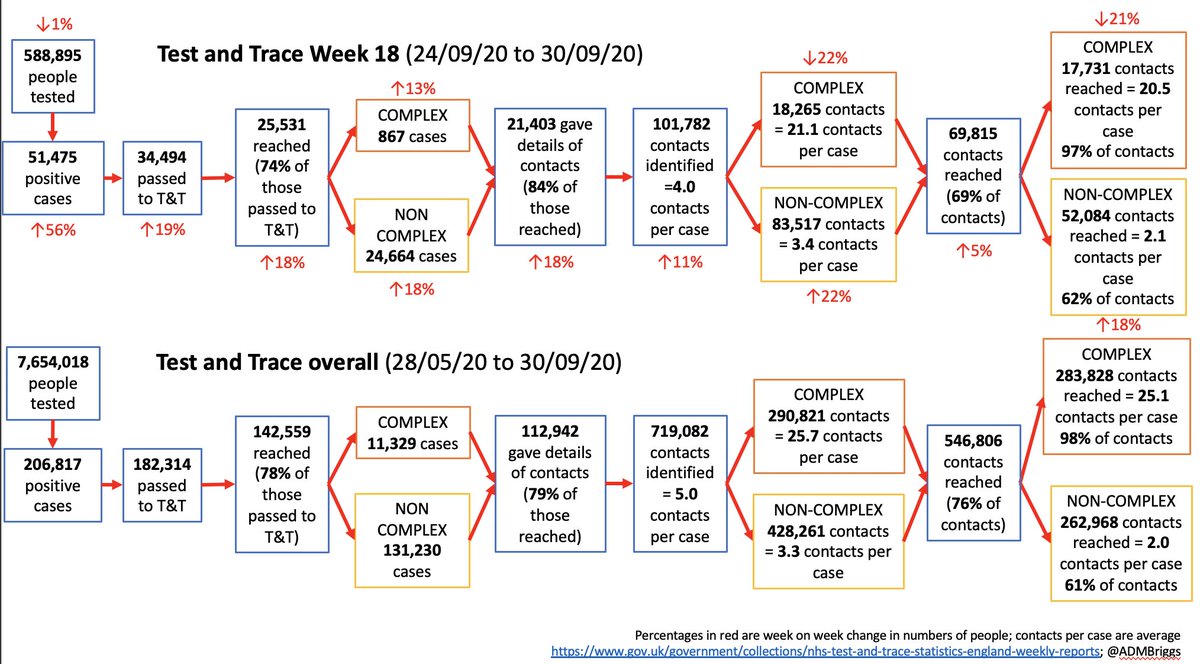
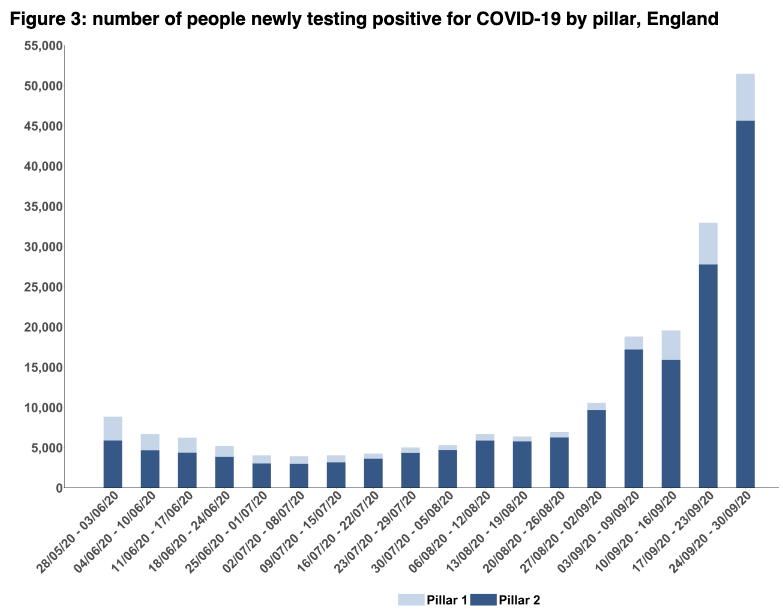
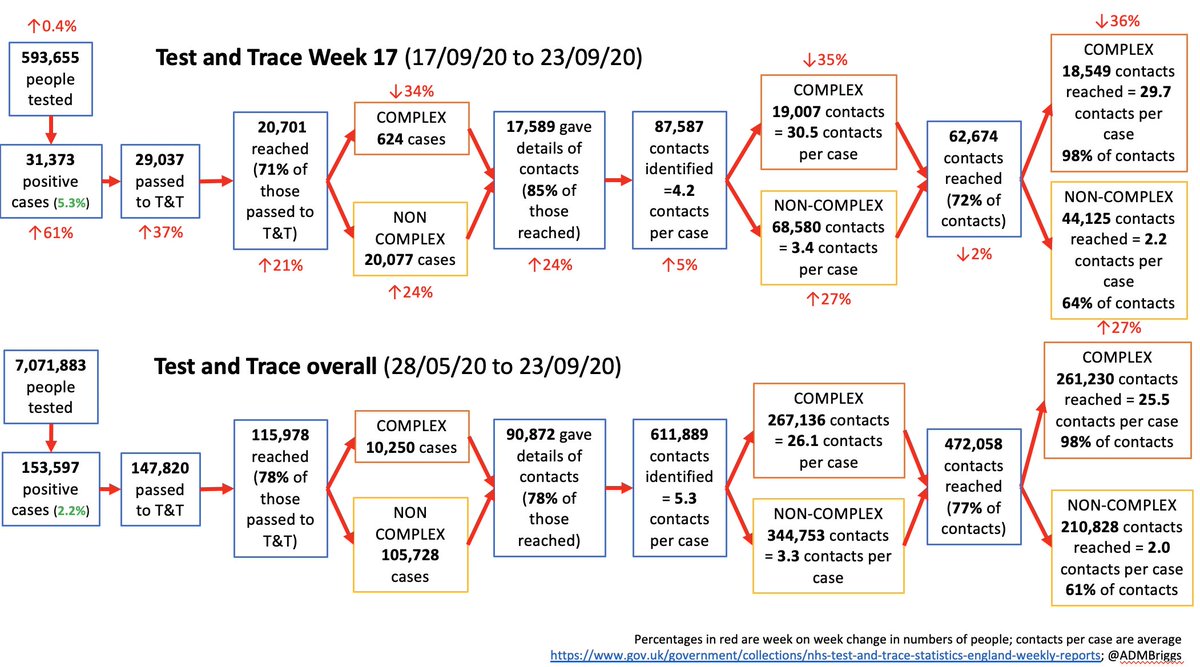
Case numbers are rising, and last week T&T only managed to reach around 75% of cases, down from an avg of around 80% in the past month or so.
However, it's getting harder for LAs to manage.
Case numbers are rising, and last week T&T only managed to reach around 75% of cases, down from an avg of around 80% in the past month or so.
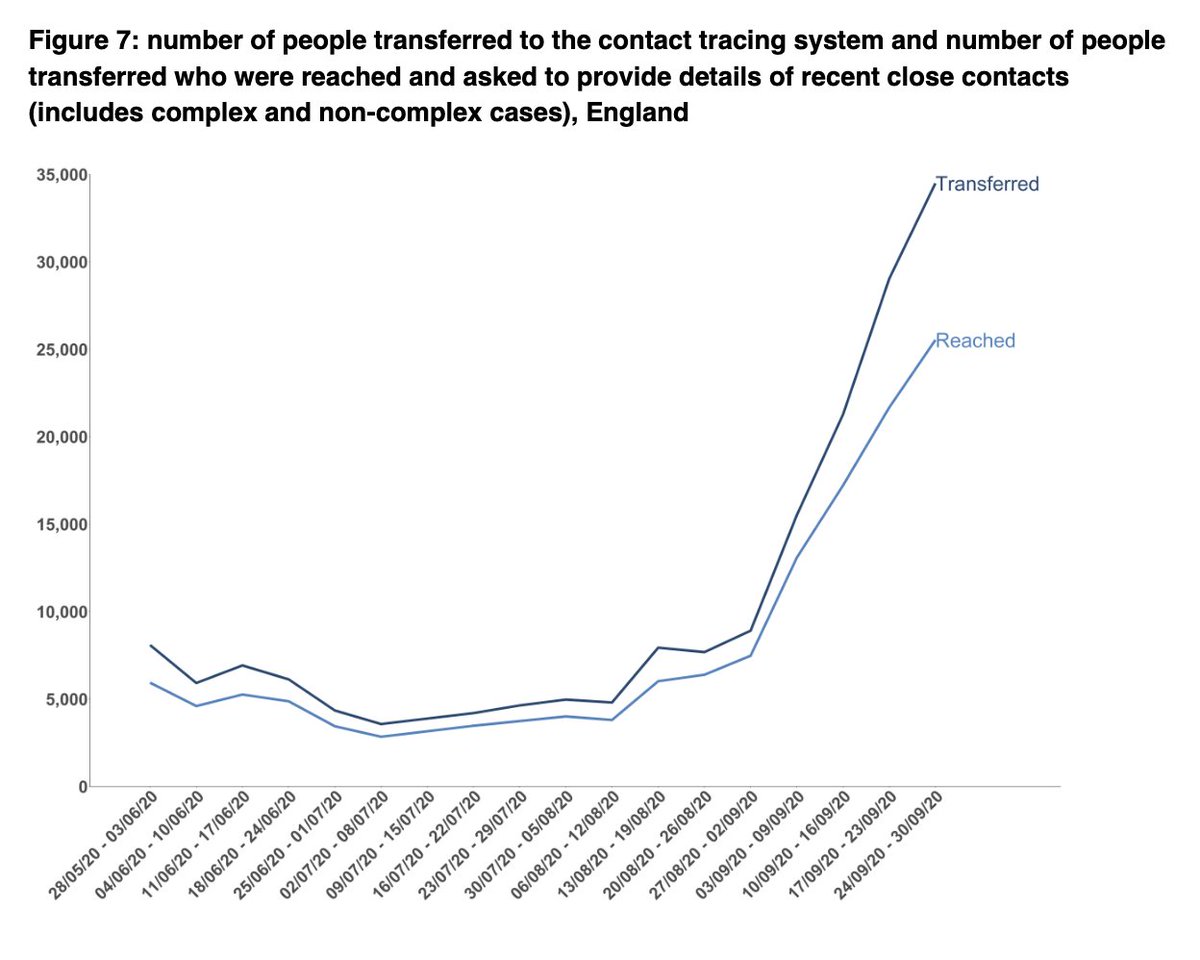
And remember that local systems generally take cases after just 24hours.
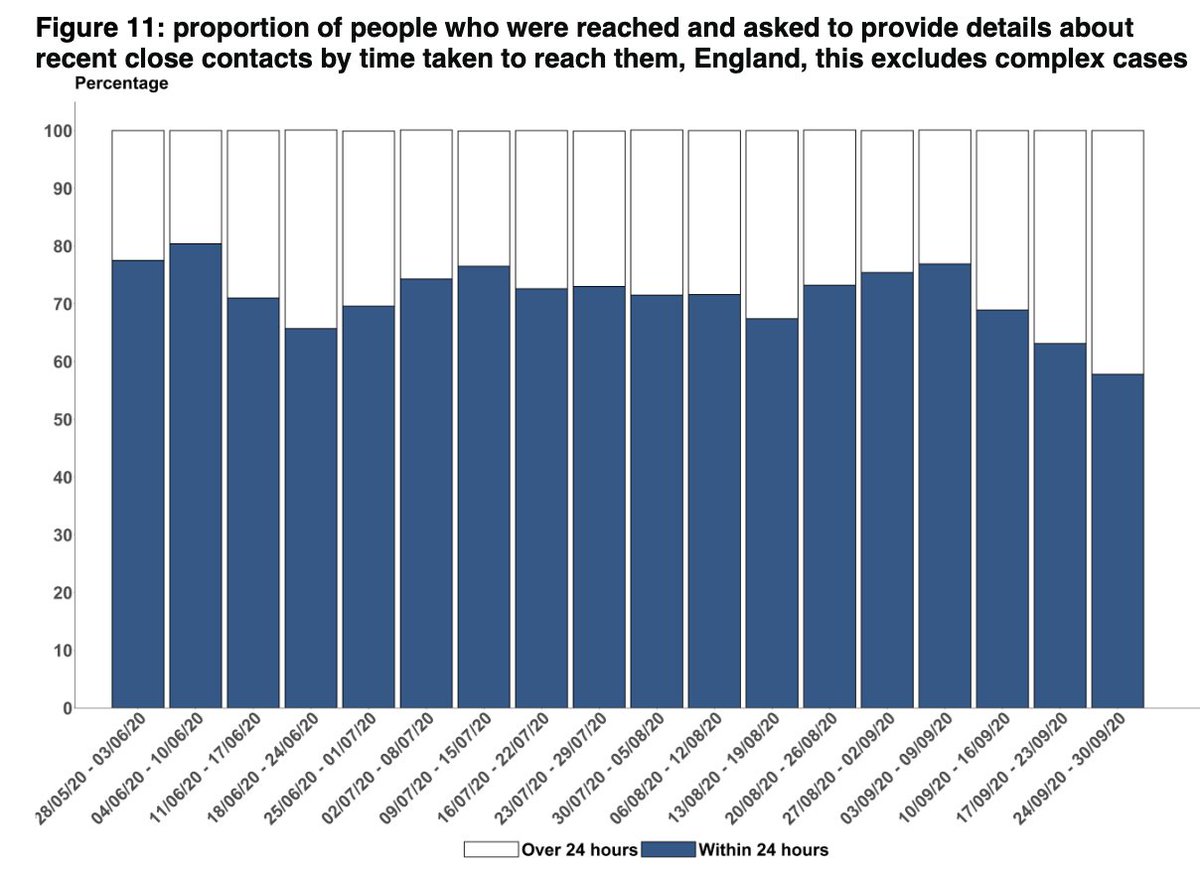
The % of cases reached with 24hrs by T&T has been really tailing off ]and now stands at 58%, down from around 75% just 3 weeks before.
The % of cases reached with 24hrs by T&T has been really tailing off ]and now stands at 58%, down from around 75% just 3 weeks before.
This kind of case load is either already unmanageable, or is getting that way. Local authorities haven't had any more money to do this.
They're working off their share of the £300m from when they developed local outbreak control plans in June.
gov.uk/government/new…
They're working off their share of the £300m from when they developed local outbreak control plans in June.
gov.uk/government/new…
The success of local contact systems depends on the national NHS Test and Trace service, it's explicitly a partnership.
Local systems can't handle all the cases, and they're not meant to.
But they're being asked to do more and more.
Local systems can't handle all the cases, and they're not meant to.
But they're being asked to do more and more.
Today, @BorisJohnson announced that those areas with the highest alert rating would receive additional £ for local test and trace.
This is v welcome, but if we want contact tracing to be 'local by default' and a true partner of the national system, then this won't be enough.
Especially is those local systems are then asked to also follow up contacts (these are currently fed back into T&T once identified).
Especially is those local systems are then asked to also follow up contacts (these are currently fed back into T&T once identified).
Instead, funding is going to be required for local authorities across the country. Not just those with the highest case numbers.
It needs happen BEFORE places get to that stage (although perhaps it's already too late for that).
It needs happen BEFORE places get to that stage (although perhaps it's already too late for that).
There will need to be significant recruitment initiatives or routes to transfer T&T staff to local gov. The money needs to be enough to cover the admin support, the HR time, the training, the supervision, the IT, etc.
And this will help with managing local cases and limiting spread/outbreaks. As contact tracing is supposed to.
But it isn't a silver bullet. Everything else still needs to happen as well.
But it isn't a silver bullet. Everything else still needs to happen as well.
But even more optimistically, it *might* just allow public health teams to start thinking about their business as usual - the smoking services, sexual health services, inequalities work, health checks, obesity prevention etc that's all been put on hold through much of this.
The legacy of COVID won't be contact tracing, it'll be the gaping inequalities in health, social, and economic opportunity left behind.
This is what local public health teams and local go do best.
And they NEED to be doing this AS WELL AS tackling COVID.
This is what local public health teams and local go do best.
And they NEED to be doing this AS WELL AS tackling COVID.
Yet long term budgets have been cut.
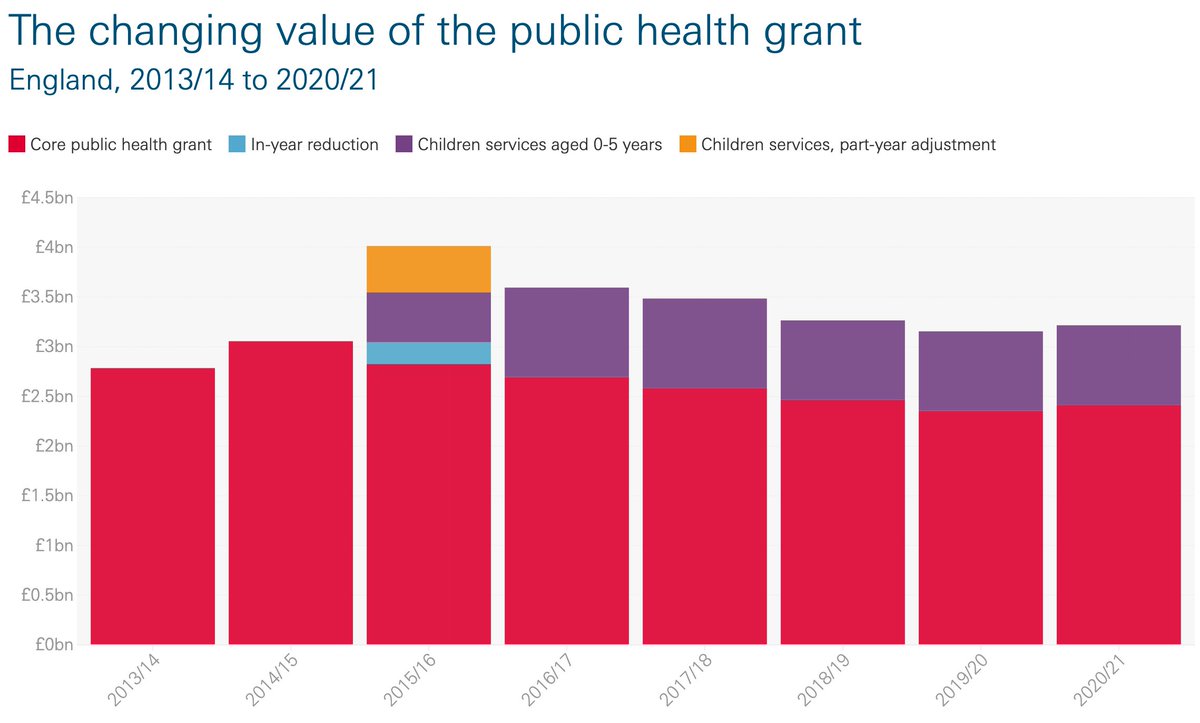
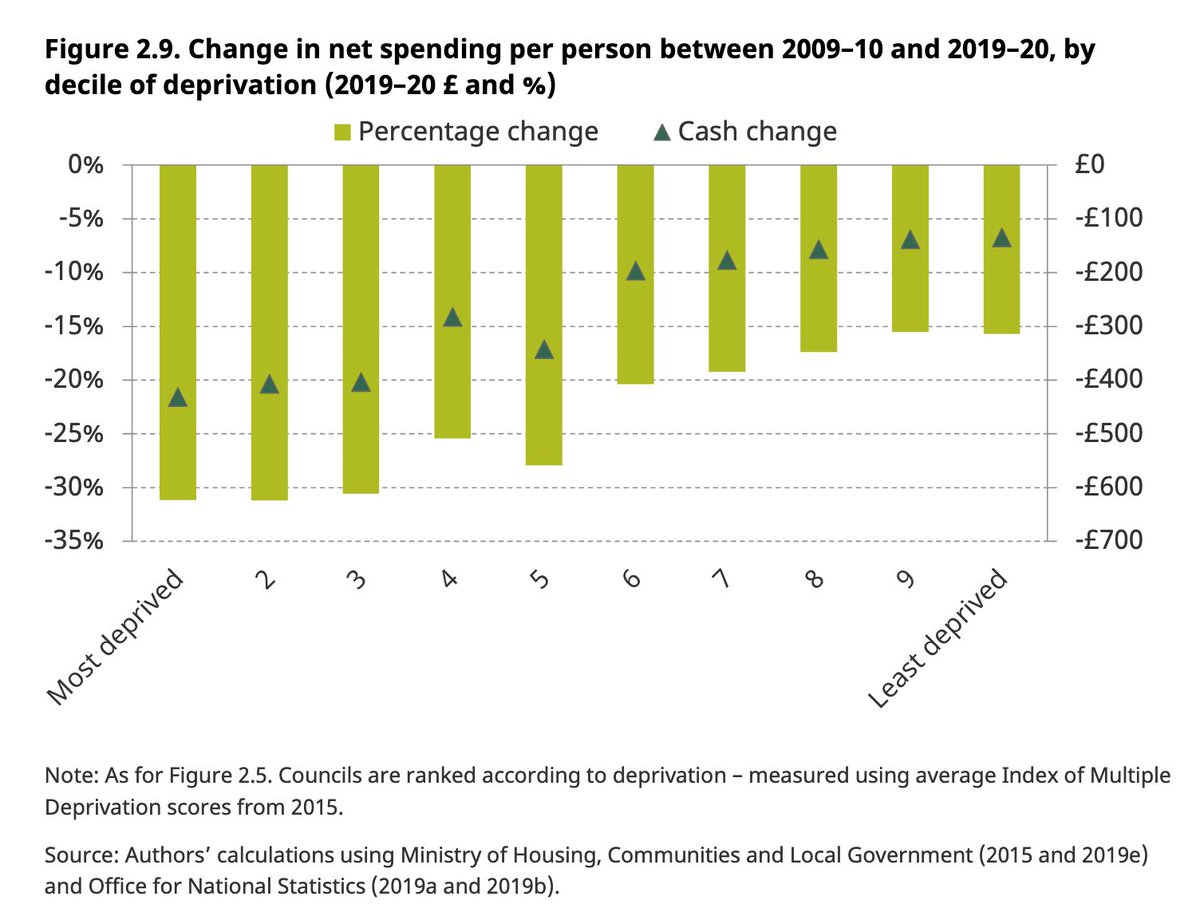
The public health grant down by nearly £1bn since 2015/16. A 17% fall in council spending on local services since 2009/10, cuts that have disproportionately affected more deprived areas.
The public health grant down by nearly £1bn since 2015/16. A 17% fall in council spending on local services since 2009/10, cuts that have disproportionately affected more deprived areas.

So whilst more welcome local financial support is being divvied out for COVID, the long term challenges remain and are getting worse.
To level up, to be local by default, means local gov can't continue to be the go-to budget line for national economic savings.
COVID shows us now more than ever why local gov and local public health teams are so critical, and why it needs urgent long term investment.
COVID shows us now more than ever why local gov and local public health teams are so critical, and why it needs urgent long term investment.
• • •
Missing some Tweet in this thread? You can try to
force a refresh