Slovakia (pop 5.5M) is attempting a mass COVID-19 screening campaign using rapid antigen tests. The public health community is going to learn a lot. Here's what I'm looking for...
1/
spectator.sme.sk/c/22519165/cor…
1/
spectator.sme.sk/c/22519165/cor…
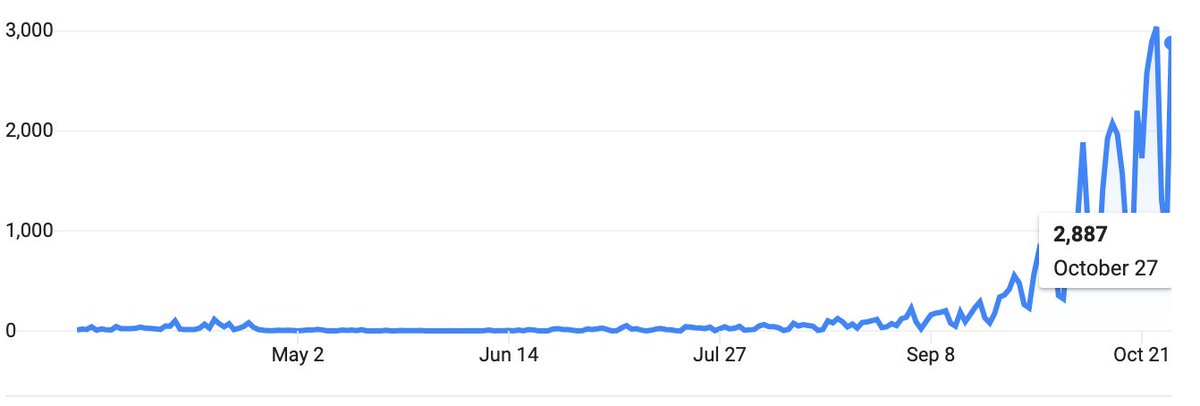
Slovakia, like Europe, is experiencing a rapid acceleration of infections & deaths, and is starting to use curfews & lockdowns.
A pilot phase tested 140K people with rapid antigen tests, found 5.5K positives (4%).
They'll test the nation over next 2 weekends! Good idea?
2/
A pilot phase tested 140K people with rapid antigen tests, found 5.5K positives (4%).
They'll test the nation over next 2 weekends! Good idea?
2/
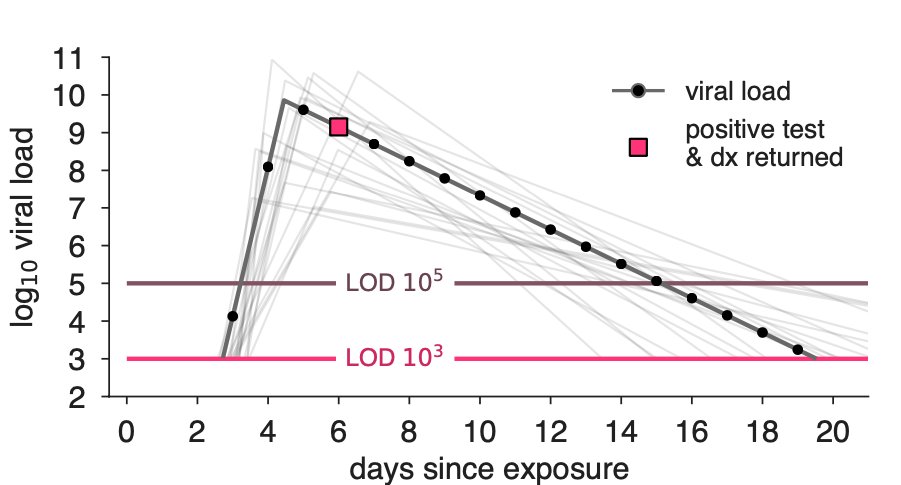
First, there are reasonable critiques of rapid Ag tests related to their sensitivity—do they miss too many infections?—and their specificity—do they falsely tell uninfected people that they're positive?
Re sensitivity: every broken transmission chain is a victory, BUT...
3/
Re sensitivity: every broken transmission chain is a victory, BUT...
3/
If a COVID+ person gets a false-negative test result, and then changes behavior—drops mask, goes to pub, etc—then the test result may have actually caused new infections!
The big Q: will screening break more transmission chains than it unintentionally creates? (I think so!)
4/
The big Q: will screening break more transmission chains than it unintentionally creates? (I think so!)
4/
The question above could be addressed through modeling, but it could also be sidestepped via better communication: a negative rapid screening test should not be a passport to 2019. Screening is a way to filter out many (not all) asymptomatic or presymptomatic infections.
5/
5/
In any case, if the Slovakian mass screening works, we should see a huge spike in cases from the screen, followed by a decline or slowing in cases thereafter due to cases averted.
@NoahHaber & ilk will have some ideas on how to do the causal epi properly. (Please, Noah?)
6/
@NoahHaber & ilk will have some ideas on how to do the causal epi properly. (Please, Noah?)
6/
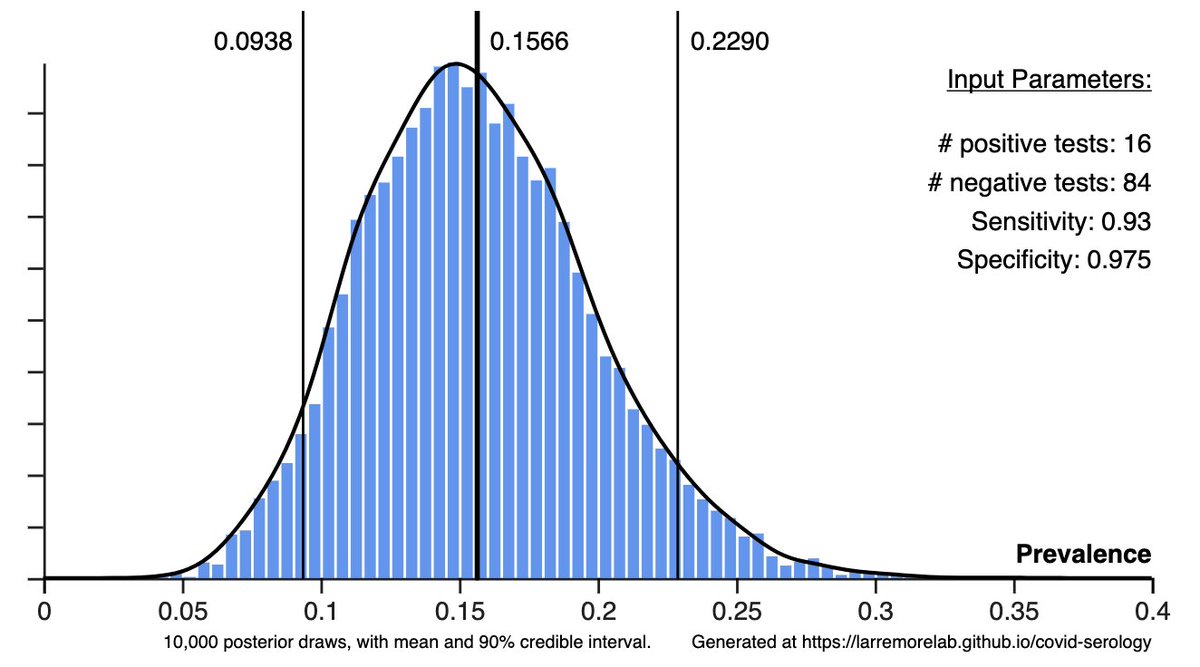
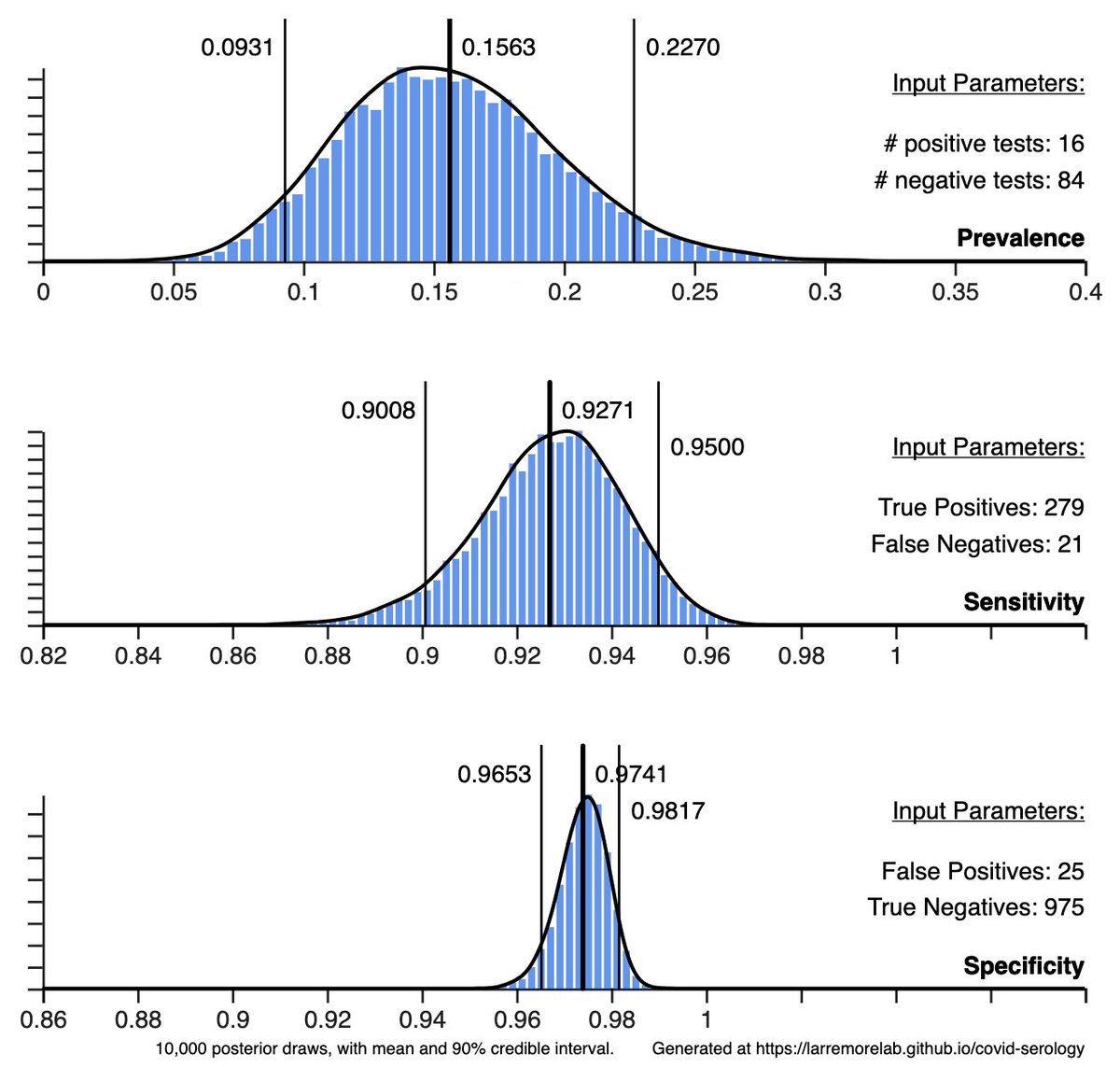
What about false positives? If prevalence is low and specificity is imperfect, it's possibly for a large fraction (even a majority) of positives to be false positives.
Unnecessary isolation days from screening? Sounds bad, but not against a counterfactual lockdown.
7/
Unnecessary isolation days from screening? Sounds bad, but not against a counterfactual lockdown.
7/
If false positive screening tests cause 1 in every 2 isolation days to be unnecessary, a lockdown at 1% prevalence causes 99 in 100 isolation days to be unnecessary.
False positive tests are a problem, to be sure, but the counterfactual matters.
8/
False positive tests are a problem, to be sure, but the counterfactual matters.
8/
I'm looking forward to seeing the outcomes of Slovakia's mass screening using rapid antigen tests.
Some have argued rapid Ag tests could be a disaster, while others argue they could be a silver bullet. The proof will be in the epi curves. Let's see what the data say.
9/9
Some have argued rapid Ag tests could be a disaster, while others argue they could be a silver bullet. The proof will be in the epi curves. Let's see what the data say.
9/9
• • •
Missing some Tweet in this thread? You can try to
force a refresh