How is diuretic efficiency changing with severity of #CKD? What is its prognostic relevance?
Read our new paper in CardioRenal Medicine!
@WilsonTangMD @BammensBert
Also thanks to Jeff Testani, Pieter Martens & Dirk Kuypers for their help with the paper...
Read our new paper in CardioRenal Medicine!
@WilsonTangMD @BammensBert
Also thanks to Jeff Testani, Pieter Martens & Dirk Kuypers for their help with the paper...

We used 3 metrics of diuretic efficiency, based on urine output, natriuresis & chloruresis.
Irrespectively of metric, loop diuretic efficiency decreased significantly from KDIGO class IV, while remaining relatively preserved in less advanced CKD.
Irrespectively of metric, loop diuretic efficiency decreased significantly from KDIGO class IV, while remaining relatively preserved in less advanced CKD.

Patterns were similar for furosemide versus bumetanide (very little patients were on torsemide, which is hardly used in Belgium). Yet, baseline characteristics were strikingly different with bumetanide users older with higher cardiovascular risk.
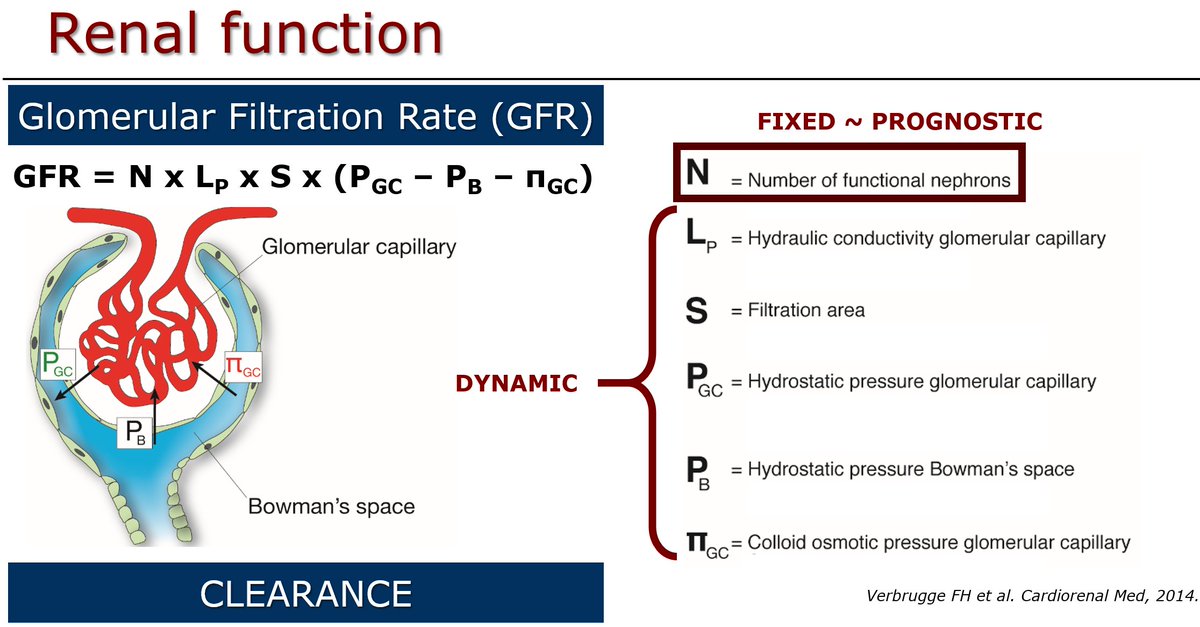
The correlation between diuretic efficiency and GFR was moderate at best, indicating there is substantial extra information captured by these metrics!

Low versus high loop diuretic efficiency, defined as a urine output ≤1000 mL versus >1000 mL per 40 mg furosemide or 1 mg bumetanide, respectively, shortened time to onset of dialysis and time to all-cause mortality both with approximately 2 years.

Forgot the link to the paper in my first tweet: karger.com/Article/Abstra… @KargerPublisher
• • •
Missing some Tweet in this thread? You can try to
force a refresh