School + CEV households: THREAD
New update yesterday for UK Guidance on shielding. Guess what stayed the same:
“Children who live with someone who is clinically extremely vulnerable, but who are not clinically extremely vulnerable themselves, should still attend school.” 1/25
New update yesterday for UK Guidance on shielding. Guess what stayed the same:
“Children who live with someone who is clinically extremely vulnerable, but who are not clinically extremely vulnerable themselves, should still attend school.” 1/25


“Should” is a euphemism for “must.”
If parents deregister, they lose their school place, must educate their child on their own from scratch, and risk denial of re-admission at their local school.
But trying to stay at school but work from home means fines and prosecution. 2/25
If parents deregister, they lose their school place, must educate their child on their own from scratch, and risk denial of re-admission at their local school.
But trying to stay at school but work from home means fines and prosecution. 2/25
https://twitter.com/SarahDRasmussen/status/1314593804633231360
Just what risk is on the table? It’s hard to estimate, but let’s try. 3 Q’s:
a) What’s the current risk of a UK child catching COVID in school?
b) What’s the accumulated effect of repeating these risks over time?
c) What’s the risk of the child transmitting at home? 3/25
a) What’s the current risk of a UK child catching COVID in school?
b) What’s the accumulated effect of repeating these risks over time?
c) What’s the risk of the child transmitting at home? 3/25
Qa is difficult to estimate accurately.
To attempt this, I’ll start with the recent over-all infection risks for UK children, and eliminate the largest non-school-related sources.
So let’s look at household secondary attack rate, also relevant to Qc. 4/25
To attempt this, I’ll start with the recent over-all infection risks for UK children, and eliminate the largest non-school-related sources.
So let’s look at household secondary attack rate, also relevant to Qc. 4/25
.@DiseaseEcology has a great thread on household secondary attack rate, including average results from meta-studies, a recent study that tested all household members including asymptomatic ones, and a discussion of various influencing factors. 5/25
https://twitter.com/diseaseecology/status/1322431687653904386
Findings:
1 Avg 18.8% hh SAR from studies counting symptomatic-to-symptomatic, but 53% from one US study on symptomatic-to-any infection.
2 Partner-to-partner SAR higher than parent-to-child. (The US study had 68%, 61%, & 45% transmission for 2, 3, & 4-person families.) 6/25
1 Avg 18.8% hh SAR from studies counting symptomatic-to-symptomatic, but 53% from one US study on symptomatic-to-any infection.
2 Partner-to-partner SAR higher than parent-to-child. (The US study had 68%, 61%, & 45% transmission for 2, 3, & 4-person families.) 6/25
https://twitter.com/diseaseecology/status/1322431696336154624
Since up to 45% of kids are asymptomatic, let’s be generous (ie assume a lot of child infection comes from parents) and use a 34% parent-to-child SAR (see below).
Average first-time parent age in UK is ~30, so avg parent of 1-2 4-16’s is 34-53, or older with more kids. 7/25
Average first-time parent age in UK is ~30, so avg parent of 1-2 4-16’s is 34-53, or older with more kids. 7/25


We next estimate the % of UK kids who were PCR-detectable on 23 Oct as a result of parent transmission.
PCR+ lasts ~8-10 days for kids, incubation ~2-14 days (usually 2-7). 34-53yo infection increased ~linearly in Oct, so let’s look 9/2 + 4 =~9 days earlier, at 14 Oct. 8/25
PCR+ lasts ~8-10 days for kids, incubation ~2-14 days (usually 2-7). 34-53yo infection increased ~linearly in Oct, so let’s look 9/2 + 4 =~9 days earlier, at 14 Oct. 8/25
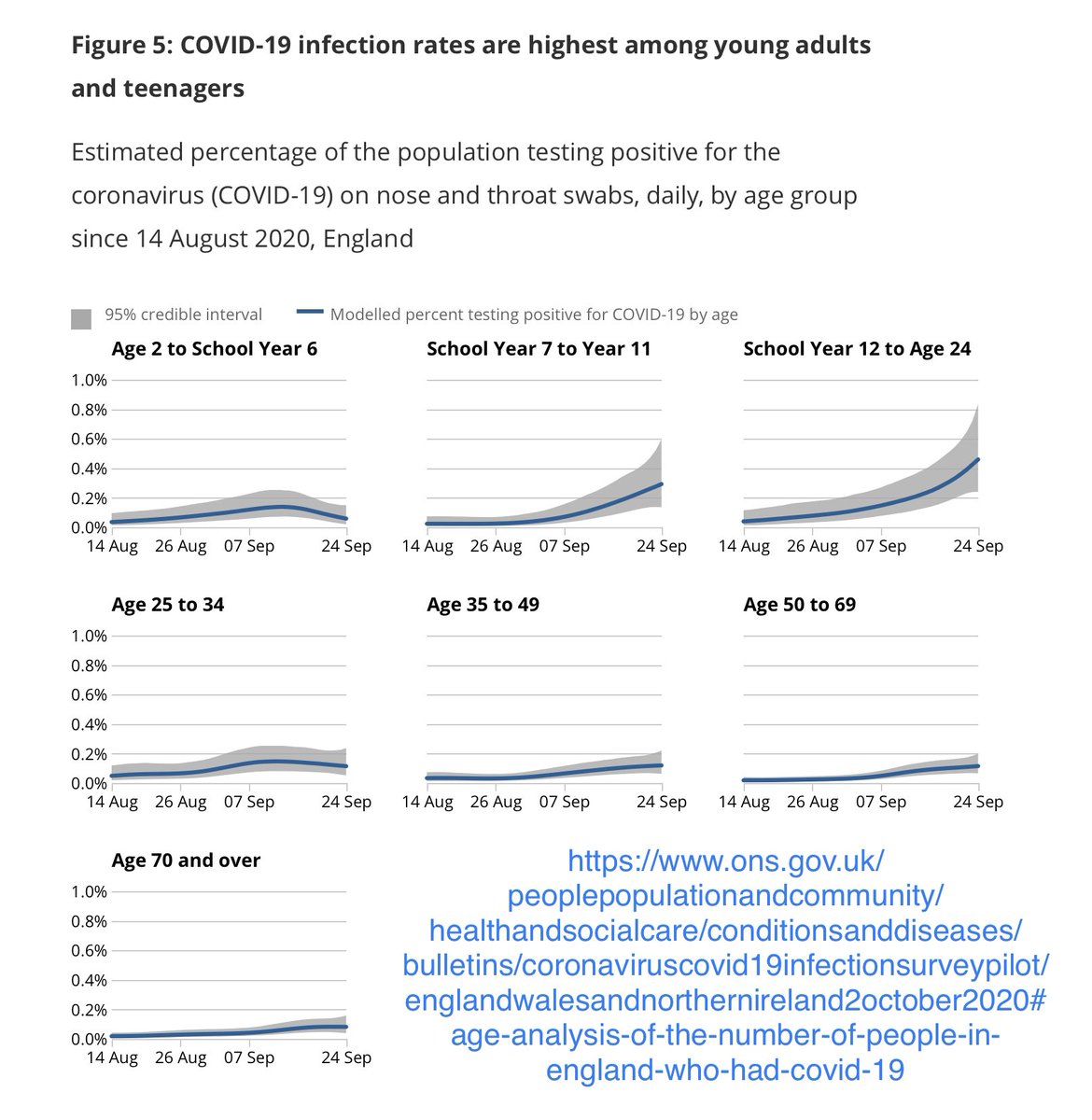
ONS estimated 14 Oct infection rates of .64% for 35-49s and .60% for 50-69s, so let’s pick the higher rate, and assume school-parents had the same infection rate as non-parents their age, so that on average .64% of parents were infectious in the relevant time window. 9/25

~77% of UK kids live with 2 carers, and we’re using a 34% parent-to-child SAR, so with the simplified approximation of independent probabilities, we get
23% x .0064 x .34 + 77% x 2 x .0064 x .34 < .39%
of 23 Oct UK kids had COVID from household adults. 10/25
23% x .0064 x .34 + 77% x 2 x .0064 x .34 < .39%
of 23 Oct UK kids had COVID from household adults. 10/25

I’m counting school-to-child-to-sibling transmission as school-sourced. The parent-to-child-to-sibling route is subsumed in parent SAR measurements.
And I’m neglecting non-school-related, non-household sources (see notes on 17/25).
So now we just subtract .39%. 11/25
And I’m neglecting non-school-related, non-household sources (see notes on 17/25).
So now we just subtract .39%. 11/25
ONS: 1.04% 2-11, 2.01% 11-16, & 2.30% 16-24 on 23 Oct, but 20-23 Oct data’s less certain, and steep for 11-16, so let’s underestimate + say 1.75% 11-16.
Subtract .39%...
➡️a 4-11yo or 11-16yo had ~a .65% or 1.36% infection risk from school in the window preceding 23 Oct. 12/25
Subtract .39%...
➡️a 4-11yo or 11-16yo had ~a .65% or 1.36% infection risk from school in the window preceding 23 Oct. 12/25

Qb: How does this risk add up over time?
That depends on how this infection-from-school risk changes over time. @IndependentSage estimate current lockdown measures (w/o school closure) will reduce R to .85, and that by 4 weeks, this will halve daily case counts. 13/25
That depends on how this infection-from-school risk changes over time. @IndependentSage estimate current lockdown measures (w/o school closure) will reduce R to .85, and that by 4 weeks, this will halve daily case counts. 13/25
https://twitter.com/independentsage/status/1322174182113857538
The mean of 1 and 1/2 is 75%, so let’s assume that for the next month, the avg infected-at-school risk per infection interval is 75% of our tweet-12 answers, or .49% and 1.02% for 4-11s and 11-16s.
And let’s conservatively assume 3 potential infection intervals per month. 14/25
And let’s conservatively assume 3 potential infection intervals per month. 14/25
With %s that low, 2nd-order effects can be neglected, making consecutive probabilities approximately additive. (For small p, p + (1-p)p ~= 2p).
So a 4-11yo has roughly a 3 x .49% = 1.5% risk of infection from school this month, and a 11-16yo has roughly a 3.1% risk. 15/25
So a 4-11yo has roughly a 3 x .49% = 1.5% risk of infection from school this month, and a 11-16yo has roughly a 3.1% risk. 15/25
If restrictions are relaxed at the end of lockdown to make R near 1 again, then for each subsequent month, the per-interval risks will be ~ .33% and .68%, and the per-month risks of infection from school will be roughly 1.0% for a 4-11yo and 2.0% for a 11-16yo. 16/25
So unless R drops much more than expected, the avg UK 4-11yo has about a 1.5% risk of being infected at school this month, and a 11-16yo has a 3.1% risk,
with risks of ~1% and 2% per month in subsequent months, depending on R values then.
Some potential sources of error: 17/25
with risks of ~1% and 2% per month in subsequent months, depending on R values then.
Some potential sources of error: 17/25

Qc: Spread to family.
For a healthy household with average COVID risk rates, the overall risk for a given person to catch COVID in any ~10-day interval is best approximated by the infection rate for that person’s demographic group, from random sampling-based estimates. 18/25
For a healthy household with average COVID risk rates, the overall risk for a given person to catch COVID in any ~10-day interval is best approximated by the infection rate for that person’s demographic group, from random sampling-based estimates. 18/25
The risk from school children is more relevant to a Clinically Extremely Vulnerable household member shielding from most other sources.
Most CEV individuals, especially immuno-suppressed ones, are more easily infected than the average person, so standard SARs don’t apply. 19/25
Most CEV individuals, especially immuno-suppressed ones, are more easily infected than the average person, so standard SARs don’t apply. 19/25
If the attack rate is 50-70% for the CEV person, then in the next month alone, they face approximately
an added .75-1.1% risk of infection for each 4-11-yo in the home,
and an added 1.5-2.1% risk of infection for each 11-16-yo in the home.
20/25
an added .75-1.1% risk of infection for each 4-11-yo in the home,
and an added 1.5-2.1% risk of infection for each 11-16-yo in the home.
20/25
The average UK school family has ~2 kids, so that’s more like a 1.5-4.2% risk.
1.5-4.2% might be an acceptable risk for breaking an arm at school.
It is not an acceptable risk for giving COVID to your mother on chemo, and potentially killing her.
21/25
1.5-4.2% might be an acceptable risk for breaking an arm at school.
It is not an acceptable risk for giving COVID to your mother on chemo, and potentially killing her.
21/25
People say these children must stay in school at all cost to ensure continuity of education and prevent growing inequality.
But in practice, denying remote school to these children forces many to deregister—removing *all* school support and creating vast inequality. 22/25
But in practice, denying remote school to these children forces many to deregister—removing *all* school support and creating vast inequality. 22/25
People also say these children should be forced to attend in-person school—wait for it—
For. Their. Mental. Health.
Because the absence of in-person lectures somehow trumps the daily high risk of bringing deadly infection home to a CEV loved one. 23/25
For. Their. Mental. Health.
Because the absence of in-person lectures somehow trumps the daily high risk of bringing deadly infection home to a CEV loved one. 23/25
Not even most adults are willing to do what these children are being forced to do.
Many healthcare workers living with CEV members have actually moved out of home to protect their loved ones. 24/25 bbc.com/news/uk-englan…
Many healthcare workers living with CEV members have actually moved out of home to protect their loved ones. 24/25 bbc.com/news/uk-englan…
The number of children in CEV households is small compared to students already temporarily remote-schooling due to temporary COVID-related isolation. There is no reason schools can’t support these other students.
This policy is counterproductive, irrational, and inhumane.
25/25
This policy is counterproductive, irrational, and inhumane.
25/25

@Parents_Utd @EmJ_Advocate @adamhamdy @Kit_Yates_Maths @chrischirp @globalhlthtwit @martinmckee @Dr2NisreenAlwan @fascinatorfun @dgurdasani1 @itosettiMD_MBA @ingridjohanna66 @McluckieAlison
Of course, I should always add to this the disclaimer that I’m a mathematician, not an epidemiologist, and I welcome corrections and adjustments from anyone more experienced.
But I’ve had so many parents contact me about this issue. I had contribute what skills I could.
But I’ve had so many parents contact me about this issue. I had contribute what skills I could.
• • •
Missing some Tweet in this thread? You can try to
force a refresh