
Let's HIT the topic 💊 Heparin-induced Thrombocytopenia (HIT)🩸!
This #tweetorial is a deep dive into Episode 43 of Run the List (RTL) on Thrombocytopenia: bit.ly/32feVfQ
Thanks @LeelaChock for covering this week’s topic!
This #tweetorial is a deep dive into Episode 43 of Run the List (RTL) on Thrombocytopenia: bit.ly/32feVfQ
Thanks @LeelaChock for covering this week’s topic!
Thrombocytopenia is a broad topic!
In Ep. 43 of RTL, Dr. Robert Stern, @NavinKumarMD, & @sonorato11 go over a general approach to thrombocytopenia 👇
Broadly, there are THREE umbrellas:
1. ⬆️ destruction
2. Splenic sequestration 💪
3. ⬇️ production
runthelistpodcast.com/s/RTL_Thromboc…
In Ep. 43 of RTL, Dr. Robert Stern, @NavinKumarMD, & @sonorato11 go over a general approach to thrombocytopenia 👇
Broadly, there are THREE umbrellas:
1. ⬆️ destruction
2. Splenic sequestration 💪
3. ⬇️ production
runthelistpodcast.com/s/RTL_Thromboc…
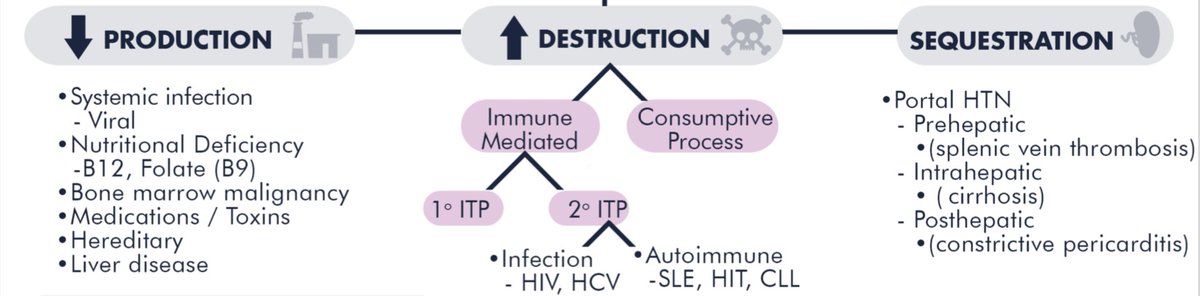
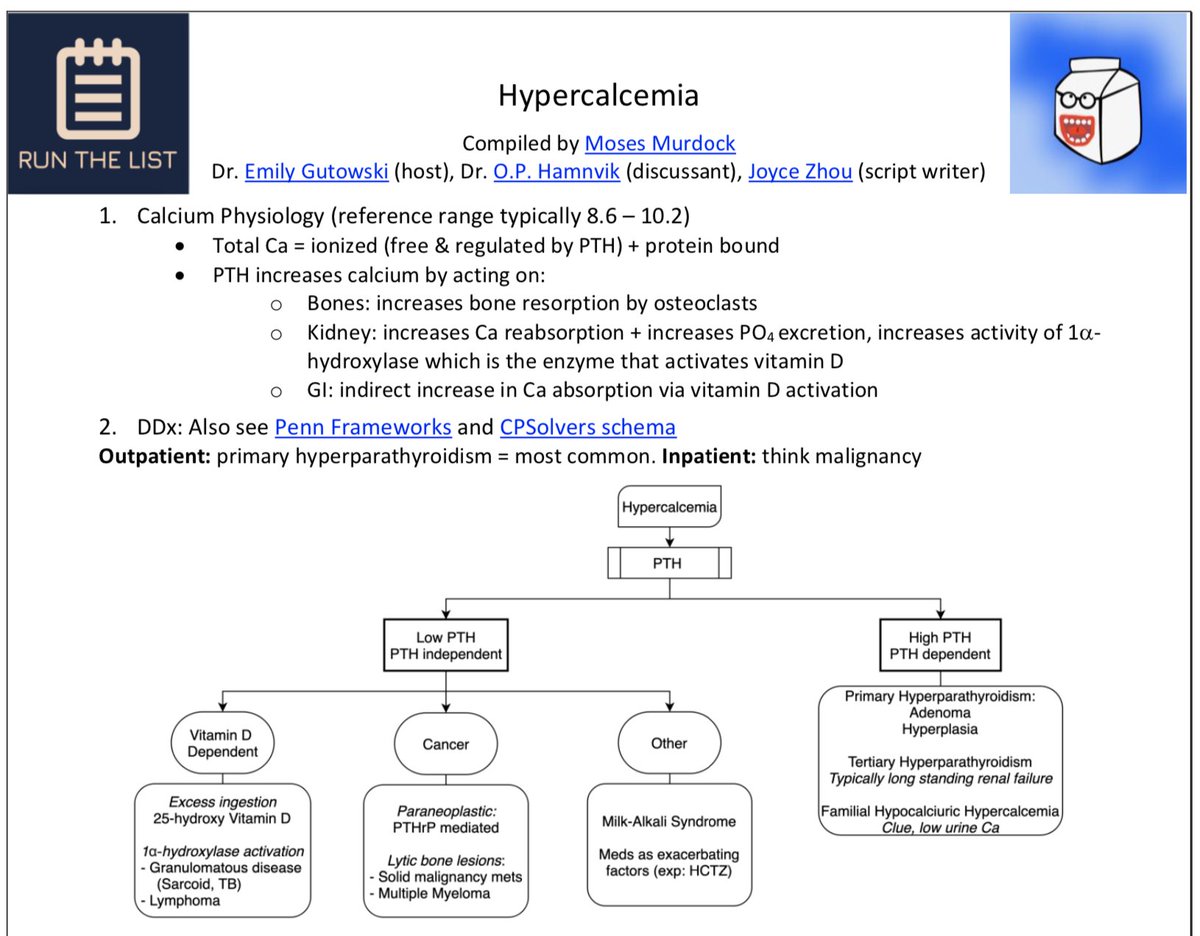
HIT (Heparin-induced thrombocytopenia), is classified under “⬆️ destruction”
HIT in-depth:
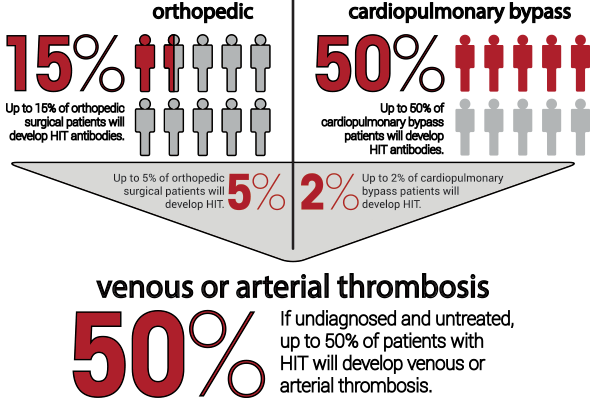
✨It is *common*, occurring in 1 out of 5,000 hospitalized patients✨
💥It’s a can’t miss dx! 50% of patients w/ HIT who are not appropriately treated go on to develop a thrombosis💥
HIT in-depth:
✨It is *common*, occurring in 1 out of 5,000 hospitalized patients✨
💥It’s a can’t miss dx! 50% of patients w/ HIT who are not appropriately treated go on to develop a thrombosis💥
HIT risk factors?
⬆️ duration/dose of heparin administration (can even happen w/ simple heparin flush!)
Type of heparin used: UFH > LMWH > fondaparinux💊
🩹Surgical, trauma, cardiopulm bypass pts at ⬆️ risk (maybe 2/2 increased heparin use, but MoA unknown)
Patient sex (F>M)
⬆️ duration/dose of heparin administration (can even happen w/ simple heparin flush!)
Type of heparin used: UFH > LMWH > fondaparinux💊
🩹Surgical, trauma, cardiopulm bypass pts at ⬆️ risk (maybe 2/2 increased heparin use, but MoA unknown)
Patient sex (F>M)
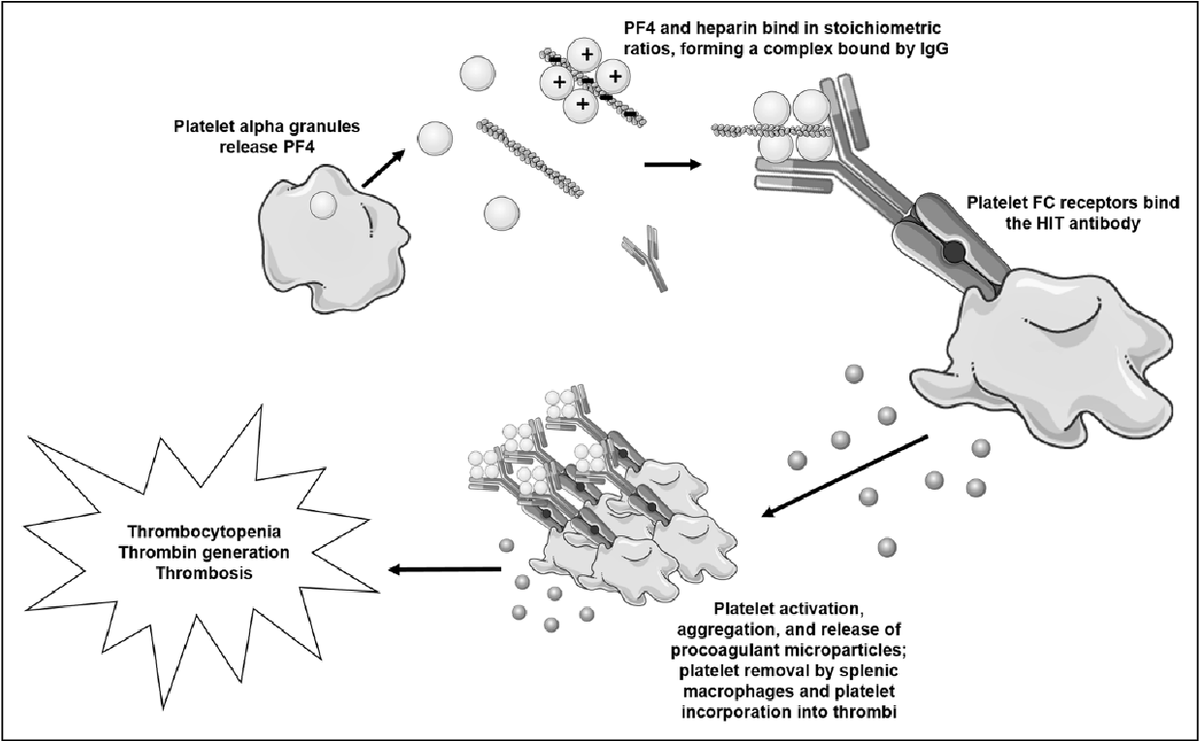
HIT mechanism:
▶ Heparin 💊 complexes w/ platelet factor 4 (PF-4), a protein released by platelets
▶ B-cells make IgG antibodies (~5-7 days after heparin exposure) to the PF4-heparin complex 🧪
▶ IgG then binds these heparin-PF4 complexes to platelets and then…
▶ Heparin 💊 complexes w/ platelet factor 4 (PF-4), a protein released by platelets
▶ B-cells make IgG antibodies (~5-7 days after heparin exposure) to the PF4-heparin complex 🧪
▶ IgG then binds these heparin-PF4 complexes to platelets and then…
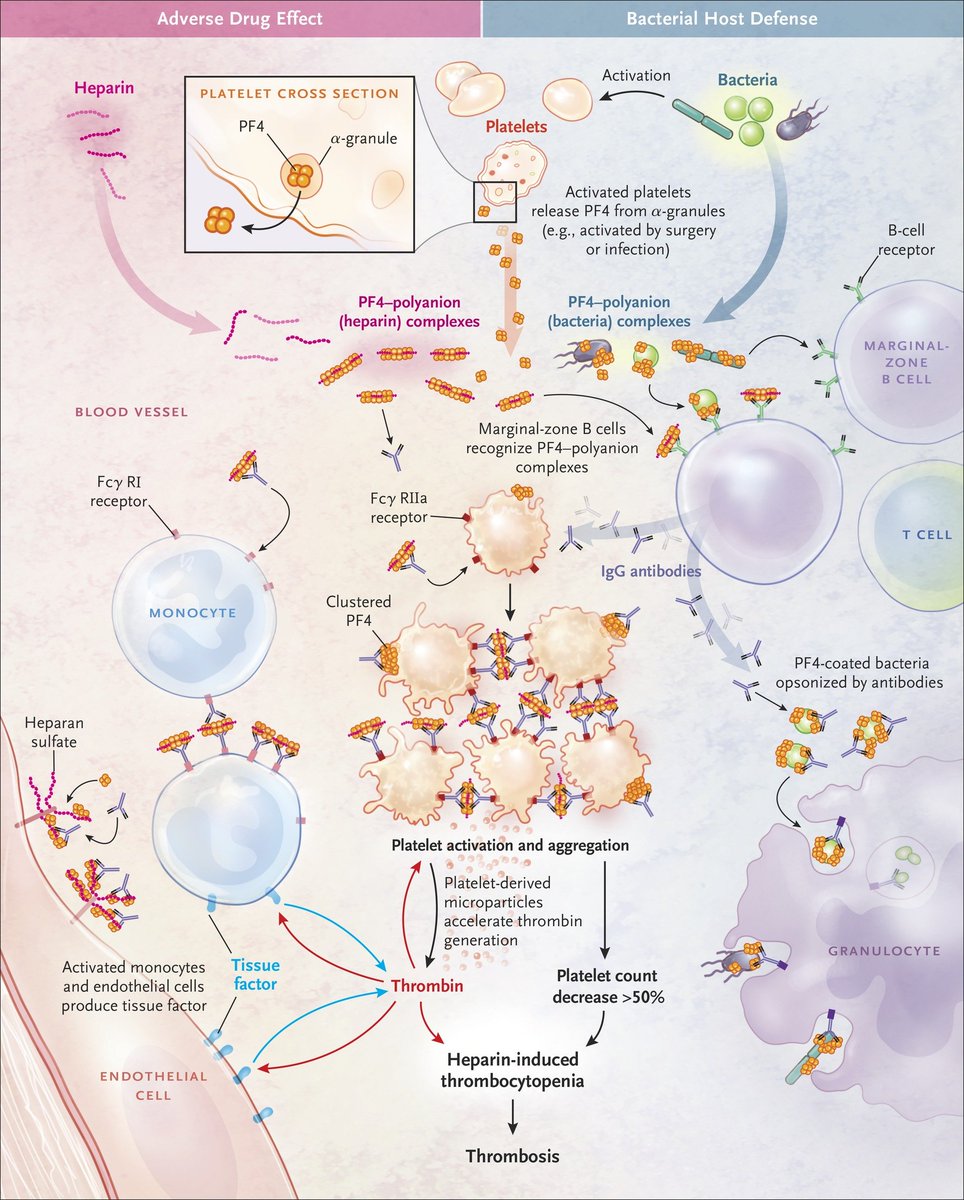
(HIT MoA cont.):
IgG-PF4-heparin complexes bind platelets causing BOTH:
1⃣Thrombocytopenia by marking the platelets for ☠️destruction☠️ via splenic macrophages (type II hypersensitivity rxn)
AND
2⃣Paradoxical PRO-thrombotic state by IgG Ab complexes 💥activating💥 platelets!
IgG-PF4-heparin complexes bind platelets causing BOTH:
1⃣Thrombocytopenia by marking the platelets for ☠️destruction☠️ via splenic macrophages (type II hypersensitivity rxn)
AND
2⃣Paradoxical PRO-thrombotic state by IgG Ab complexes 💥activating💥 platelets!
Sequelae include:
🔴Thrombocytopenia to ~50-80k (usually >20K)
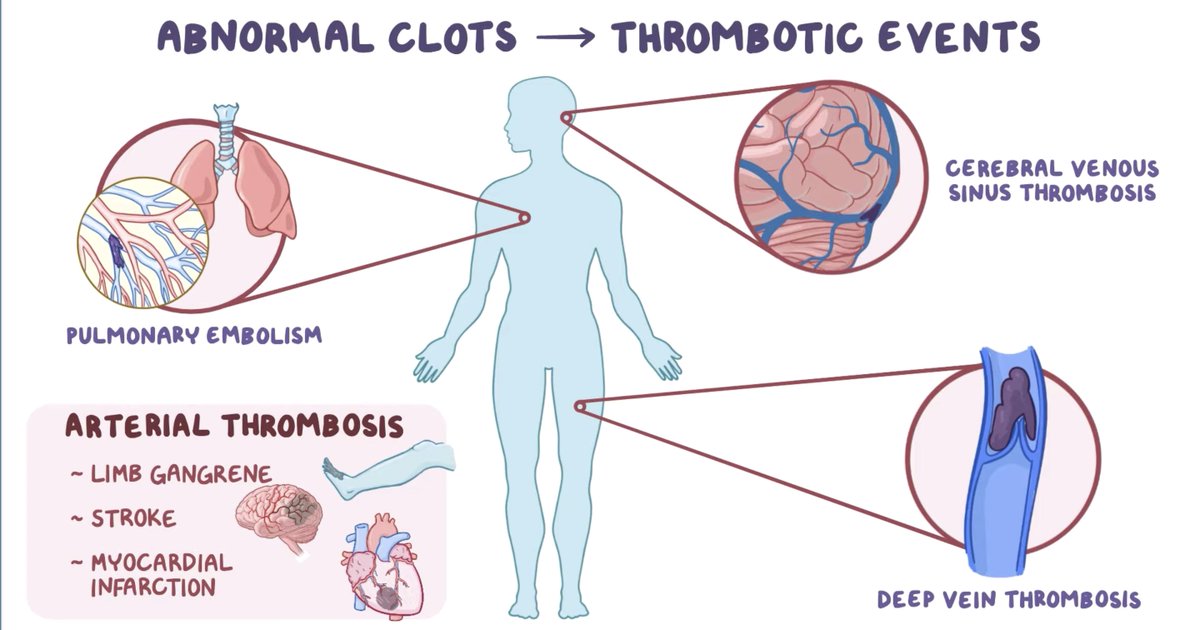
🟠Paradoxical thrombosis (venous > arterial), despite thrombocytopenia!
🟡(Rarely) anaphylaxis; HIT Ab may activate leukocytes
🟢Skin necrosis at *heparin injection sites* (seen below) immediately suggests HIT! 🩺
🔴Thrombocytopenia to ~50-80k (usually >20K)
🟠Paradoxical thrombosis (venous > arterial), despite thrombocytopenia!
🟡(Rarely) anaphylaxis; HIT Ab may activate leukocytes
🟢Skin necrosis at *heparin injection sites* (seen below) immediately suggests HIT! 🩺

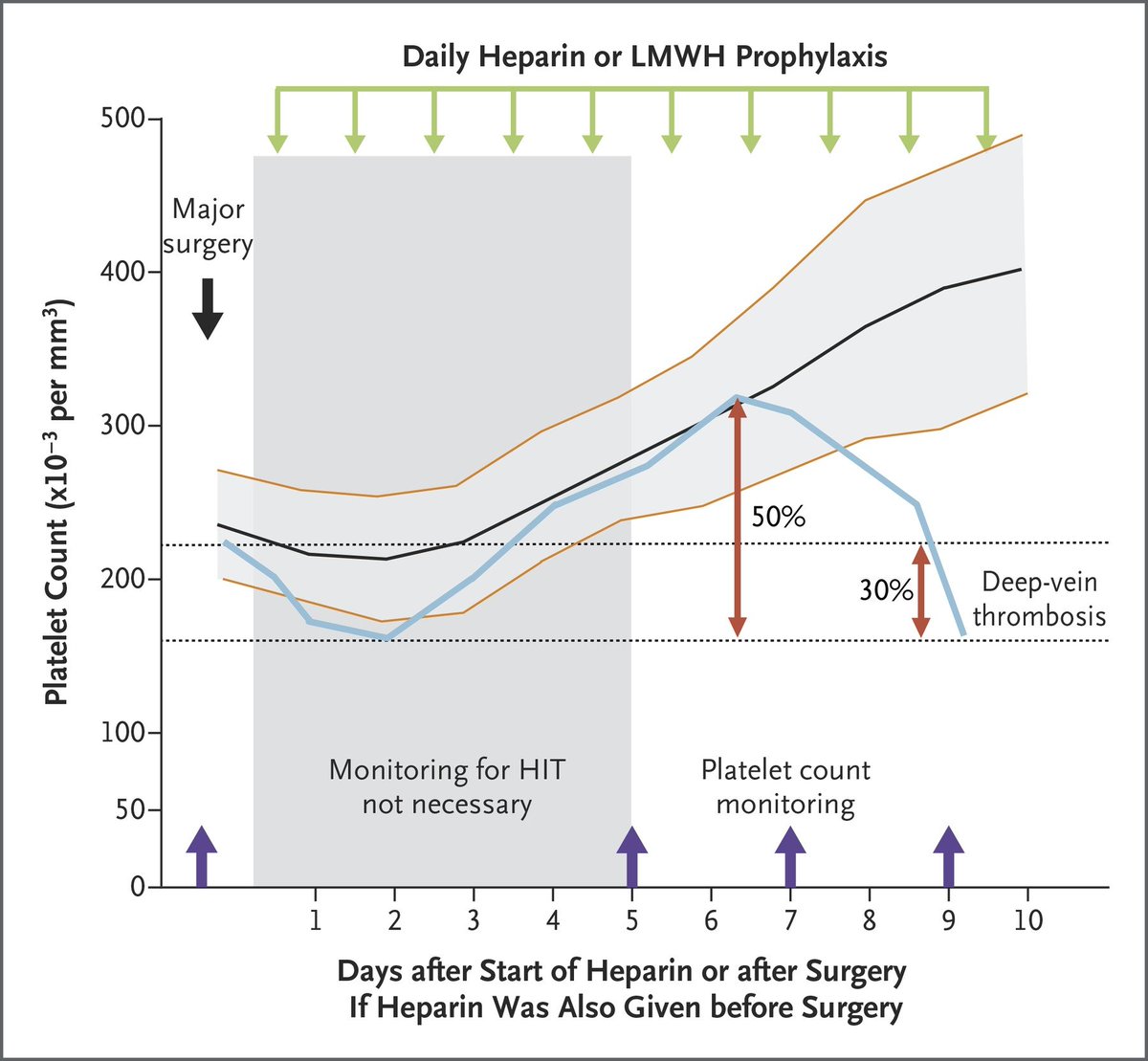
Let’s review timing ⏰ of HIT!
Suppose heparin is given on day 0:
🔸d0-d1 = Rapid 50% drop (pt already has IgG Ab 2/2 heparin exposure w/i last 3 months)
🔹d5-d7 = Rapid 50% drop (no prior heparin exposure)
🔸d7-d14 after heparin withdrawal = Rapid drop ("delayed-onset HIT")
Suppose heparin is given on day 0:
🔸d0-d1 = Rapid 50% drop (pt already has IgG Ab 2/2 heparin exposure w/i last 3 months)
🔹d5-d7 = Rapid 50% drop (no prior heparin exposure)
🔸d7-d14 after heparin withdrawal = Rapid drop ("delayed-onset HIT")
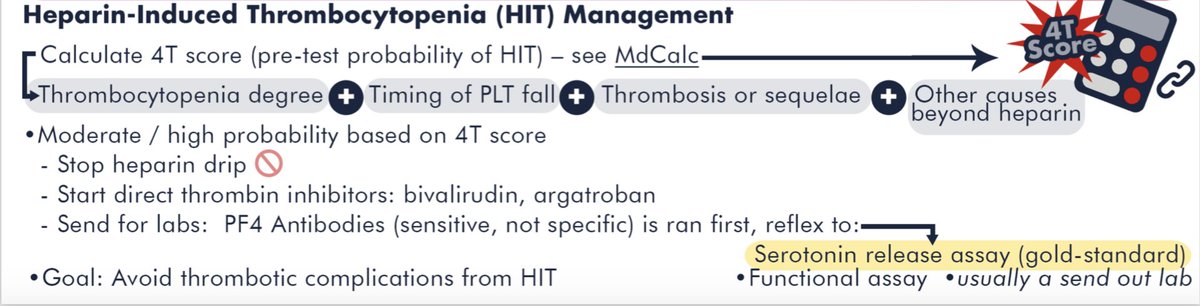
If suspecting HIT calculate a "4-T score"
The 4 T's are:
📌Thrombocytopenia
📌Timing ⌚️ of Onset
📌Thrombosis
📌oTher causes of Thrombocytopenia.
A LOW score (<4 points) has a very HIGH negative predictive value (NPV) of 97 to 99%, and essentially *rules out* HIT
The 4 T's are:
📌Thrombocytopenia
📌Timing ⌚️ of Onset
📌Thrombosis
📌oTher causes of Thrombocytopenia.
A LOW score (<4 points) has a very HIGH negative predictive value (NPV) of 97 to 99%, and essentially *rules out* HIT
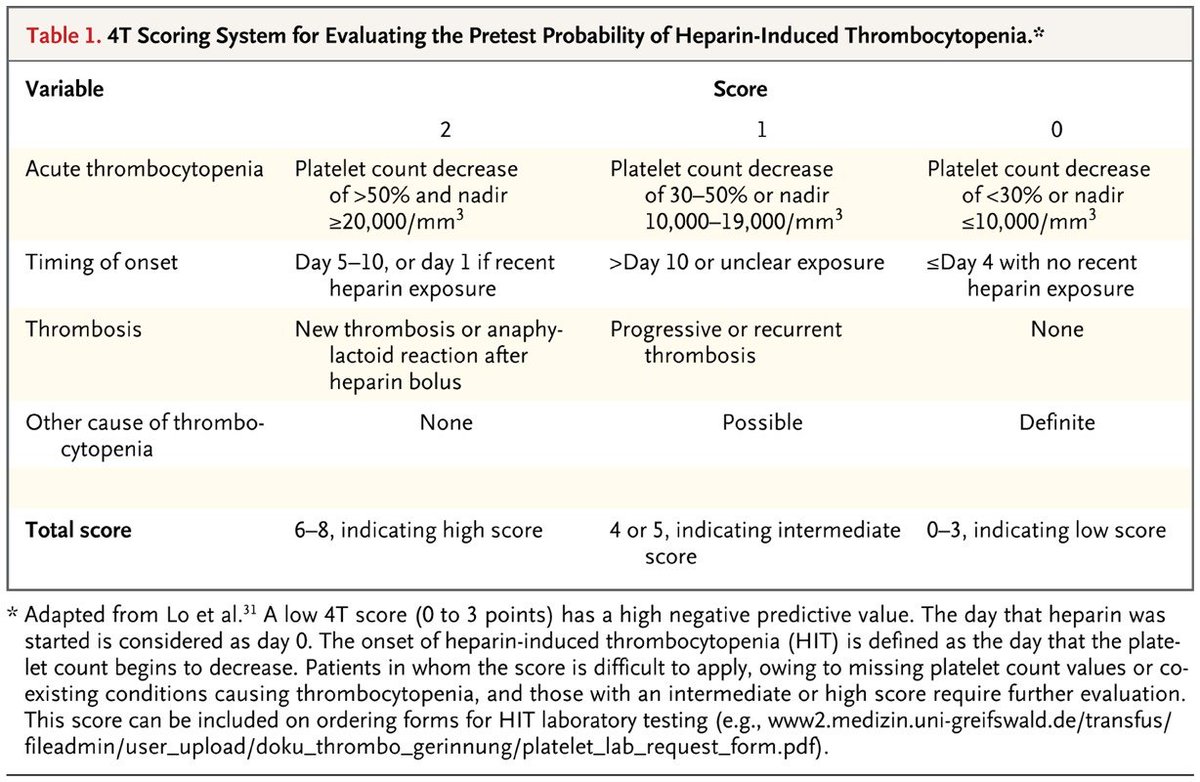
The positive predictive value (PPV) of a 4-T score of 4-5 is 10-20%, but a score >=6 is 40-80%
A 4-T score >=4 requires:
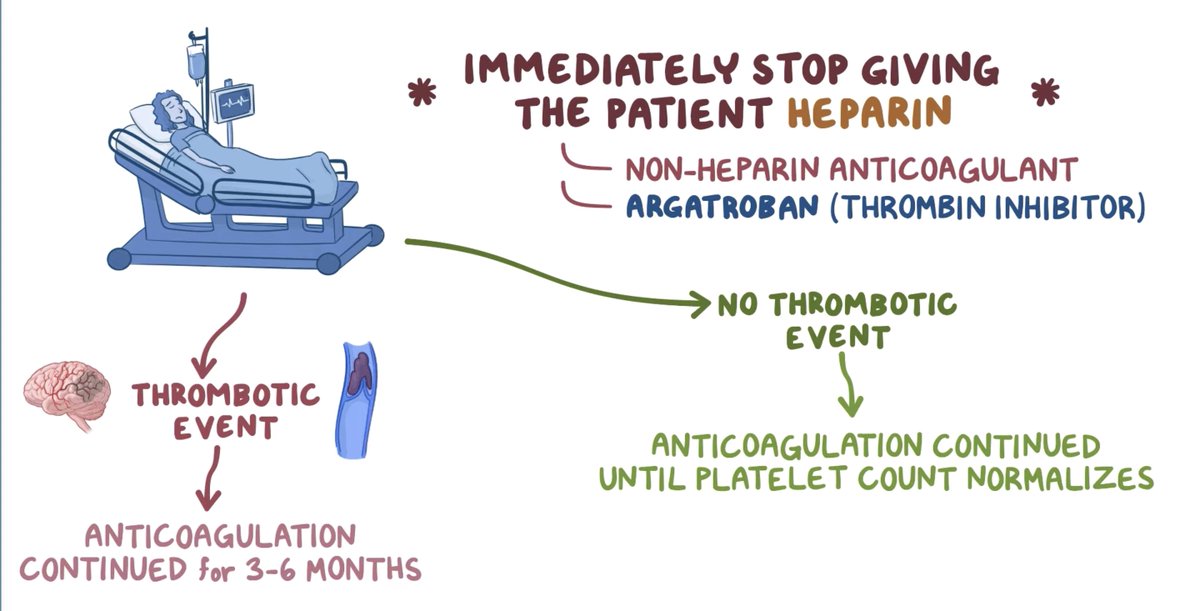
1⃣Stopping all heparin products immediately 🛑!
2⃣An Anti–PF4–heparin ELISA test 🧪
3⃣Starting therapeutic NON-heparin anticoagulation (e.g. Argatroban 💊)
A 4-T score >=4 requires:
1⃣Stopping all heparin products immediately 🛑!
2⃣An Anti–PF4–heparin ELISA test 🧪
3⃣Starting therapeutic NON-heparin anticoagulation (e.g. Argatroban 💊)

Anti-PF4 test has high NPV (98-99%), but low PPV
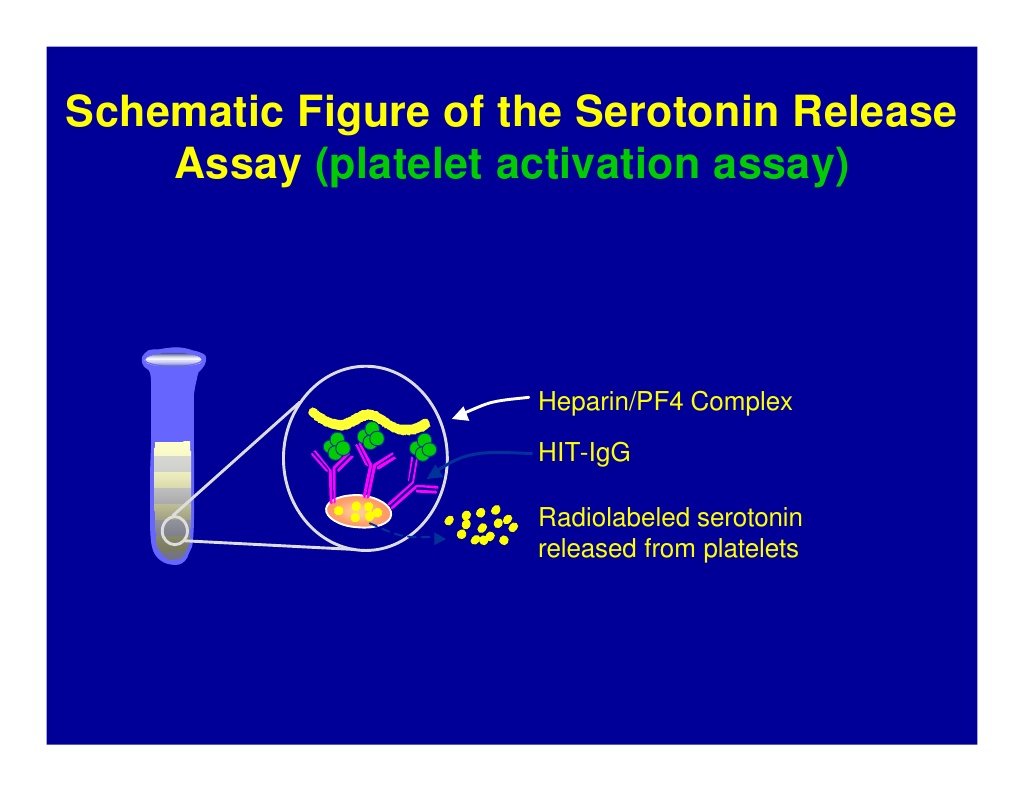
a ➕ anti-PF4 result requires confirmation w/ *gold standard functional test*: serotonin release assay (SRA)
How does SRA work?
If pt's serum has active heparin-PF4 IgG Ab ➡️ activate donor platelets ➡️ 💥 releasing serotonin 💥
a ➕ anti-PF4 result requires confirmation w/ *gold standard functional test*: serotonin release assay (SRA)
How does SRA work?
If pt's serum has active heparin-PF4 IgG Ab ➡️ activate donor platelets ➡️ 💥 releasing serotonin 💥
All pts w/ suspected or confirmed HIT need therapeutic (non-heparin) anticoagulation (AC)!
Why💊?
HIT Abs activate platelets➡️clots despite thrombocytopenia
For HIT: continue AC until platelet count >150K
For HIT-related clot: continue AC for 3 months (like any provoked clot)
Why💊?
HIT Abs activate platelets➡️clots despite thrombocytopenia
For HIT: continue AC until platelet count >150K
For HIT-related clot: continue AC for 3 months (like any provoked clot)
[on AC]
@ASH_hematology suggests the following tx as initial anticoagulants in acute HIT🩸:
📝Argatroban, bivalirudin, fondiparinux, danaparoid, or a DOAC
💊Argatroban or bivalirudin = short half-lives (!)
⌛️Short half-lives = indicated for critically ill or bleeding risk pts
@ASH_hematology suggests the following tx as initial anticoagulants in acute HIT🩸:
📝Argatroban, bivalirudin, fondiparinux, danaparoid, or a DOAC
💊Argatroban or bivalirudin = short half-lives (!)
⌛️Short half-lives = indicated for critically ill or bleeding risk pts

If pt is on warfarin, 🛑hold warfarin🛑 & reverse with IV Vitamin K 🥦
Seems strange right?
◾️Warfarin has been shown to paradoxically WORSEN the hypercoagulable state in HIT 😱
◽️Once platelet count stabilizes, can re-start warfarin 👍
Seems strange right?
◾️Warfarin has been shown to paradoxically WORSEN the hypercoagulable state in HIT 😱
◽️Once platelet count stabilizes, can re-start warfarin 👍
in SUM:
1) HIT complexes both activate *and* deplete platelets (thrombocytopenia)
2) Use the 4-T score🧮 to assess for HIT
3) If >=4 🛑heparin products, start non-heparin anticoagulation (not warfarin!), & send labs
4) Have a low threshold to look for thrombotic complications
1) HIT complexes both activate *and* deplete platelets (thrombocytopenia)
2) Use the 4-T score🧮 to assess for HIT
3) If >=4 🛑heparin products, start non-heparin anticoagulation (not warfarin!), & send labs
4) Have a low threshold to look for thrombotic complications
REFs (1/2):
[1]theawkwardyeti.com/comic/blood-cl…
[2]runthelistpodcast.com/s/RTL_Thromboc…
[3]
[4]aruplab.com/testing/HIT
[5]nejm.org/doi/full/10.10…
[6]semanticscholar.org/paper/Heparin-…
[7]uptodate.com/contents/clini…
[8]nejm.org/doi/full/10.10…
[9]nejm.org/doi/full/10.10…
[1]theawkwardyeti.com/comic/blood-cl…
[2]runthelistpodcast.com/s/RTL_Thromboc…
[3]
[4]aruplab.com/testing/HIT
[5]nejm.org/doi/full/10.10…
[6]semanticscholar.org/paper/Heparin-…
[7]uptodate.com/contents/clini…
[8]nejm.org/doi/full/10.10…
[9]nejm.org/doi/full/10.10…
REFs (2/2):
[11]slideshare.net/skyecreativeon…
[12]
[13a]ashpublications.org/bloodadvances/…
[13b]jahjournal.org/viewimage.asp?…
[15]runthelistpodcast.com/s/RTL_Thromboc…
[11]slideshare.net/skyecreativeon…
[12]
[13a]ashpublications.org/bloodadvances/…
[13b]jahjournal.org/viewimage.asp?…
[15]runthelistpodcast.com/s/RTL_Thromboc…
@MedTweetorials @CPSolvers @COREIMpodcast @CuriousClinPod @DxRxEdu @Rabihmegeha @tony_breu
@connors_md @DavidSteensma
@connors_md @DavidSteensma
• • •
Missing some Tweet in this thread? You can try to
force a refresh










{kind=link}