
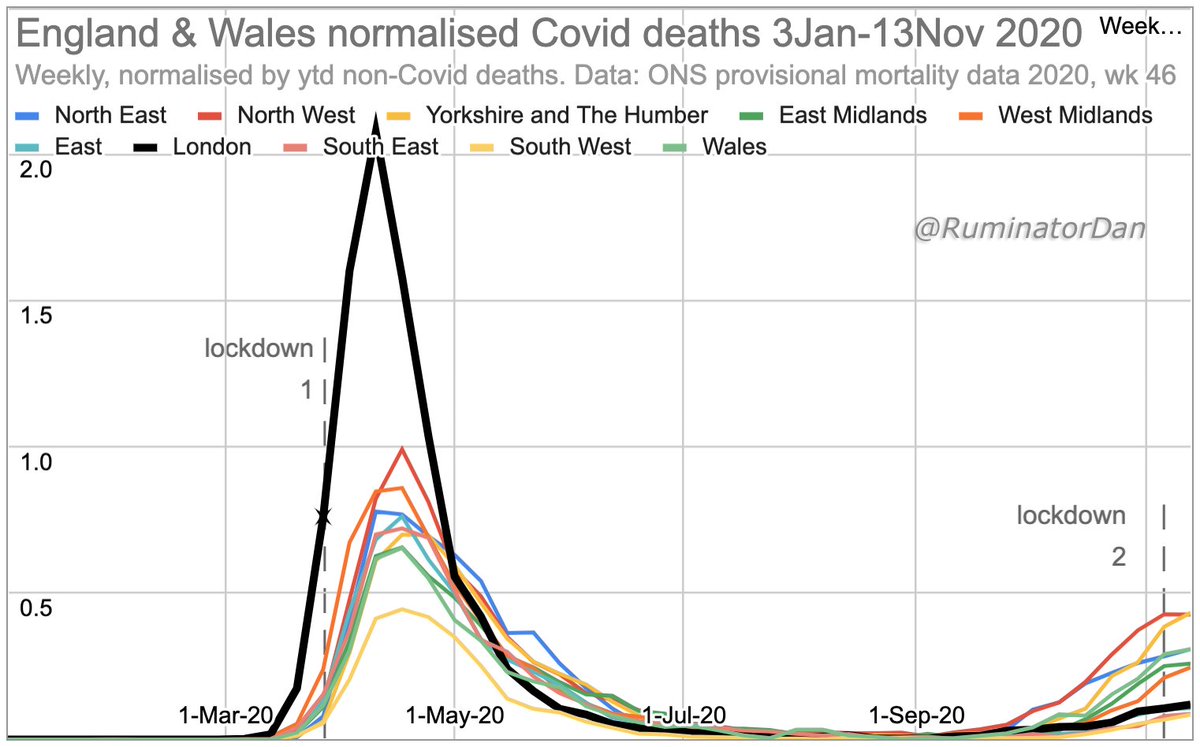
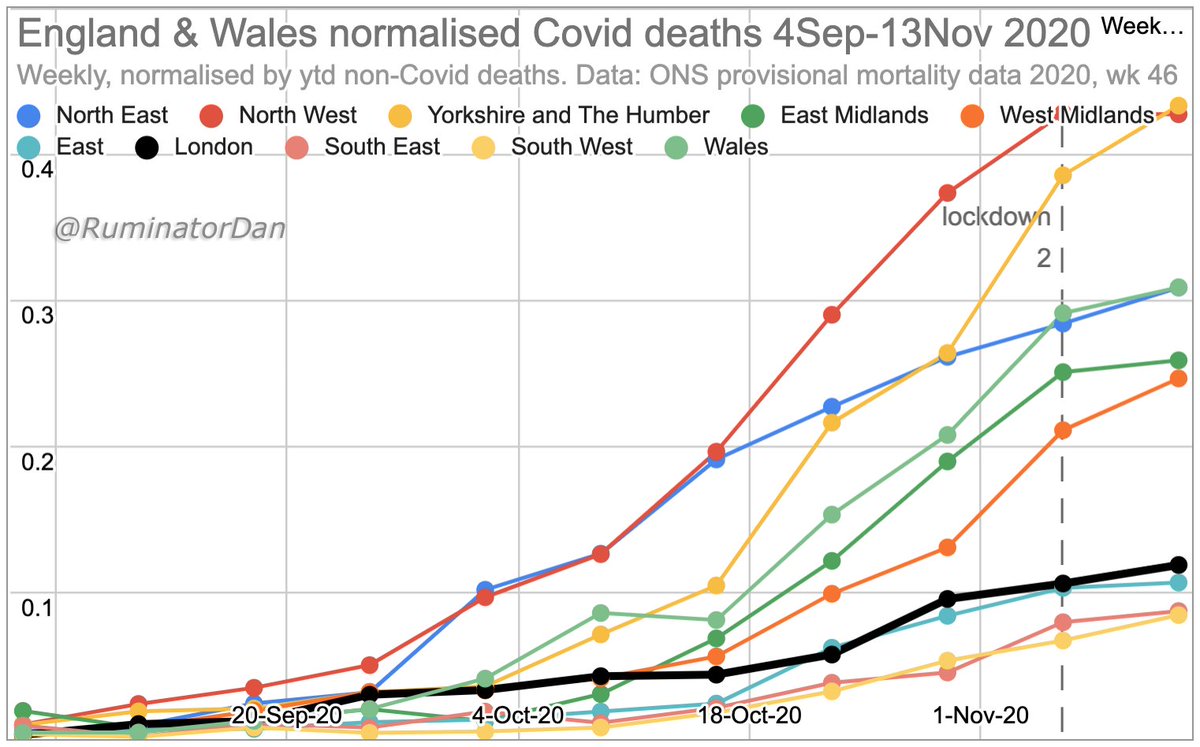
_England & Wales Autumn Covid deaths show regional heterogeneity. London, in particular, is interesting_
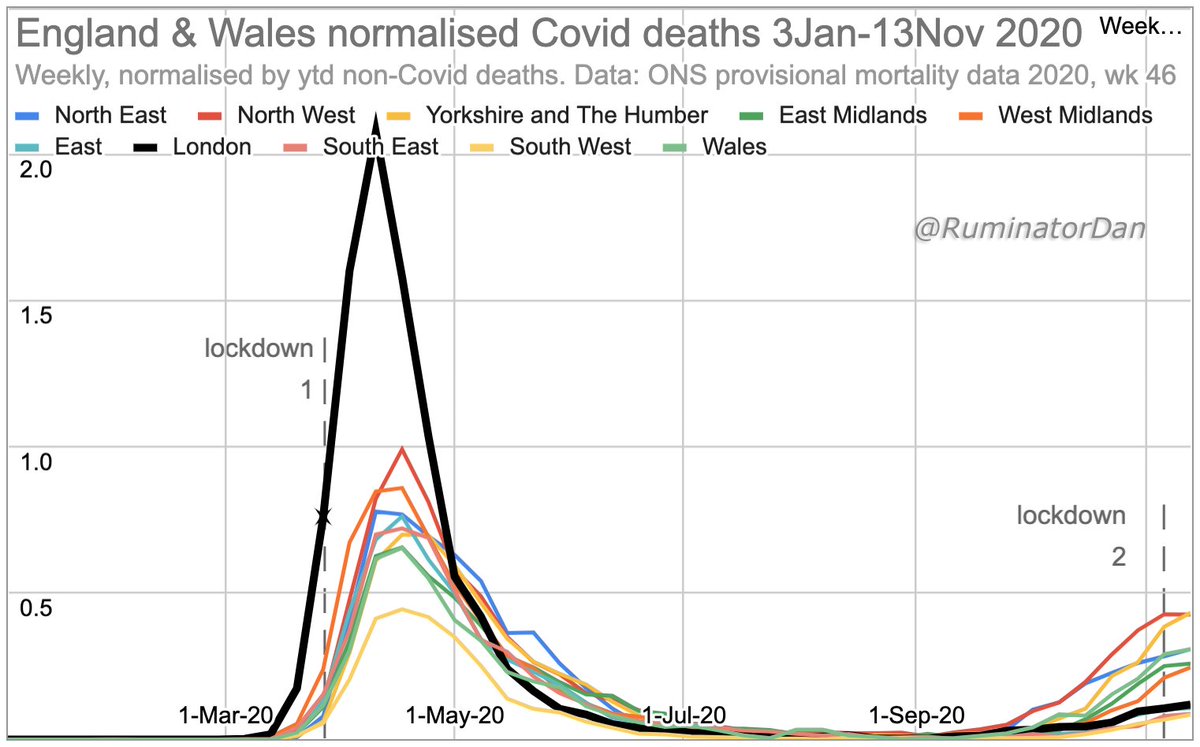
London's more severe & earlier spring growth may well explain why it has, to date, seen less of an autumn rise.
[Charts normalised by ytd non-covid deaths.]
[27Nov2020_1]
London's more severe & earlier spring growth may well explain why it has, to date, seen less of an autumn rise.
[Charts normalised by ytd non-covid deaths.]
[27Nov2020_1]
The generally held belief is that only a small percentage of people have so far been infected by SARS-CoV-2 & that the vast majority remain susceptible to infection - hence all the measures taken.
There are, however, reasons & evidence suggesting that this is not the case.
There are, however, reasons & evidence suggesting that this is not the case.
If the vast majority of people were still susceptible, one would expect growth everywhere. However, autumn rises have varied greatly across regions.
London especially, given its nature (crowding etc) would be expected to show aggressive growth, as it did in spring.
It has not.
London especially, given its nature (crowding etc) would be expected to show aggressive growth, as it did in spring.
It has not.
The past provides a clue as to the reason.
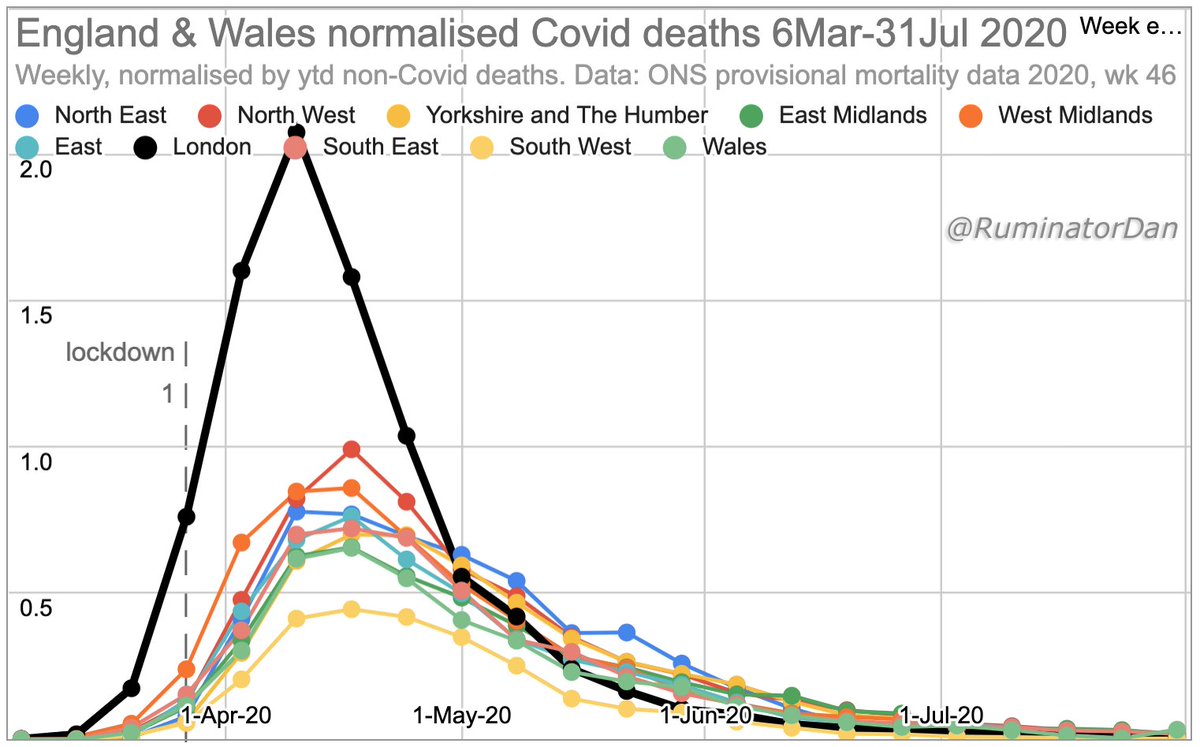
London's spring rise in Covid deaths was the most aggressive: not only faster & larger than other regions, but also earlier. When lockdown was implemented, it was already well along in its epidemic curve. Deaths peaked soon after.
London's spring rise in Covid deaths was the most aggressive: not only faster & larger than other regions, but also earlier. When lockdown was implemented, it was already well along in its epidemic curve. Deaths peaked soon after.
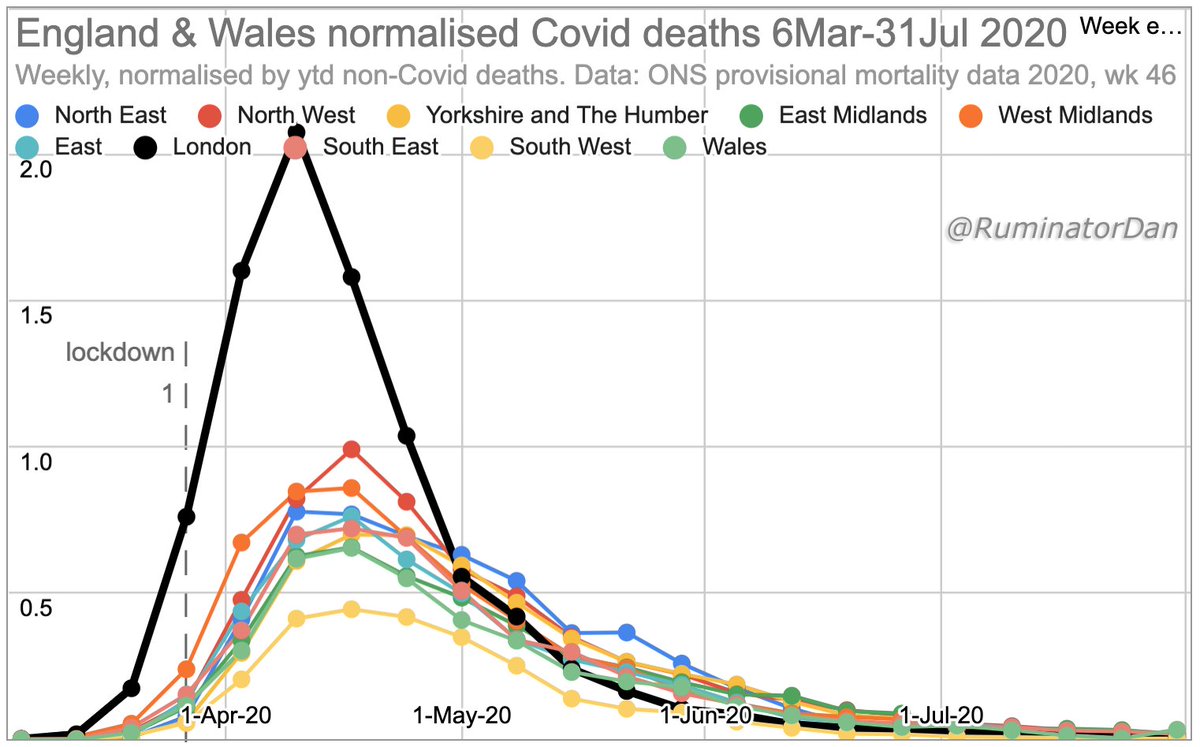
Given that the average time lag between infection & death is a number of weeks, it is clear that London's infections had already peaked before lockdown.
Therefore infections - & deaths - did not decline because of lockdown. They declined naturally.
Therefore infections - & deaths - did not decline because of lockdown. They declined naturally.
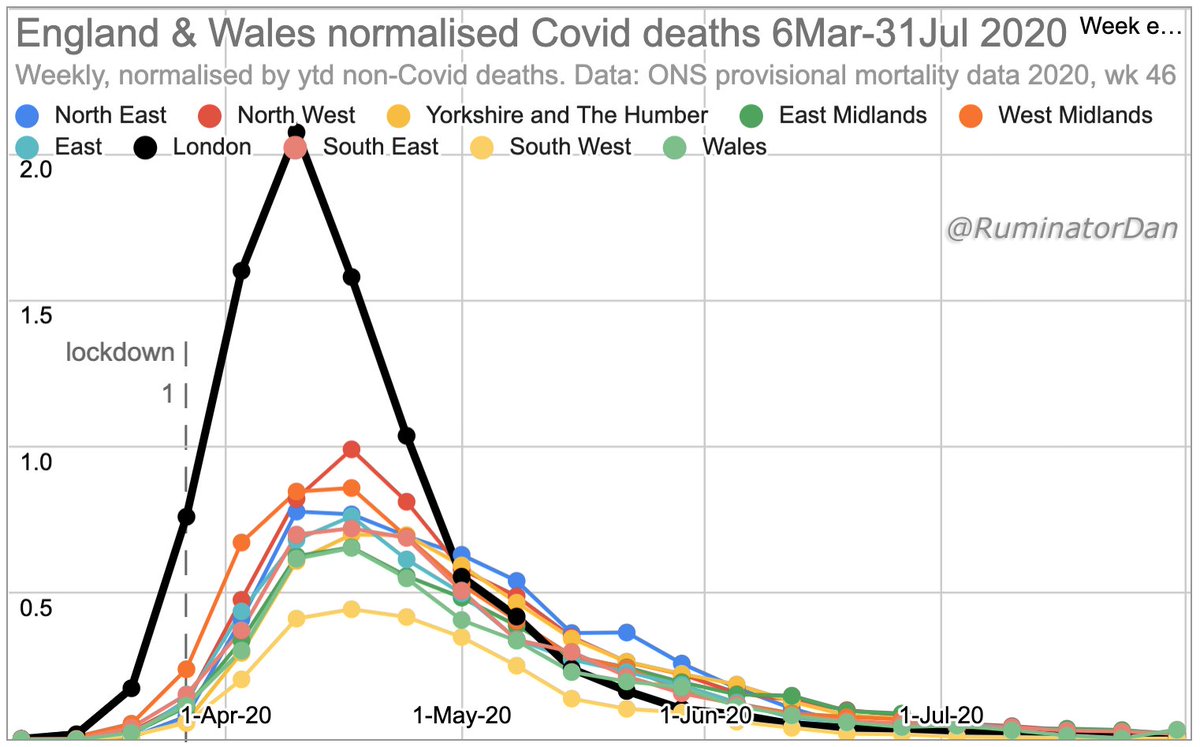
It would appear that, in London, the virus largely ran its natural course, with too few susceptible people then remaining (due to infections &/or pre-existing immunity) to enable substantial new growth.
Infections -& deaths- can still occur. But not a repeat of spring.
Infections -& deaths- can still occur. But not a repeat of spring.

The other regions were also well along in their curves at the time of lockdown - remembering again that infections run well ahead of deaths - but a little less so than London.
It would seen feasible that the lockdowns in those regions did prevent a minority of infections from occurring in the spring. This would mean that enough susceptible people then remained to allow growth in infections later.
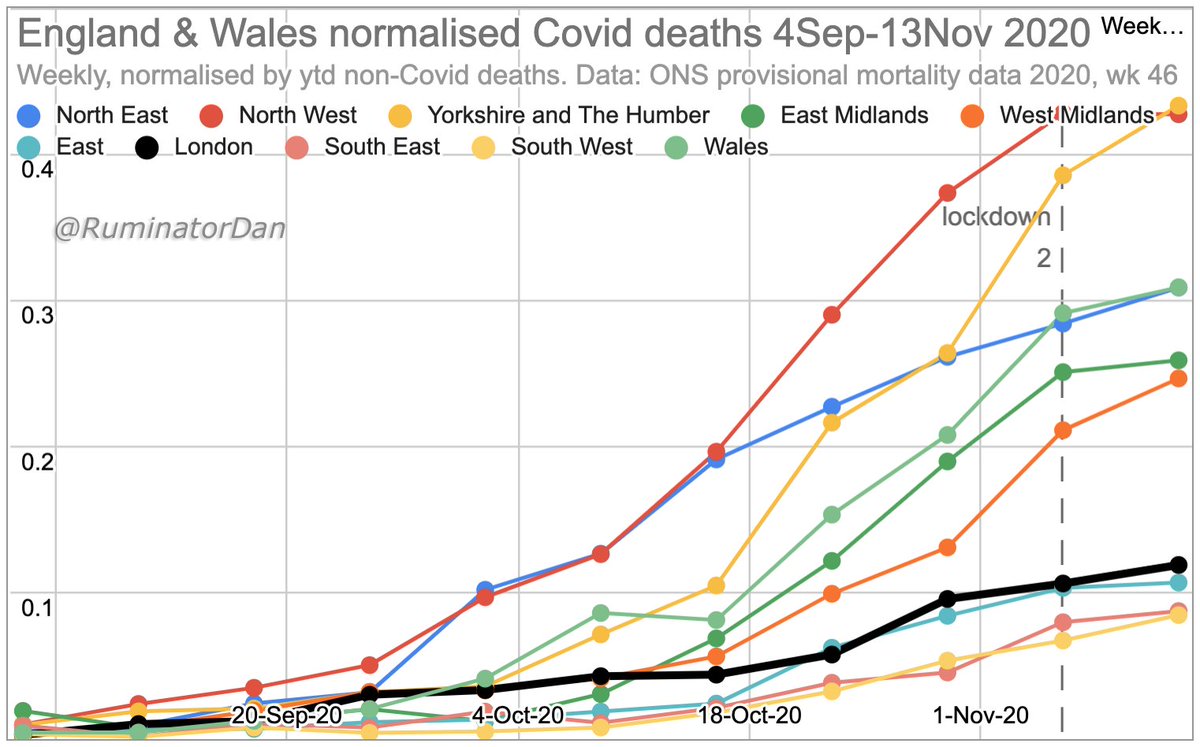
Hence, while infections appear to have increased in many regions, there is significant variation. London, by far the worst affected region in the spring, has been, to date, one of the least affected in the autumn.
Another, critical, point emerges from this:
As London (& many other locations) show, the virus, while nasty & tragic for many, appears to result in far fewer total deaths than generally predicted, e.g. 500k were predicted for the UK without measures (ICL, March 2020).
As London (& many other locations) show, the virus, while nasty & tragic for many, appears to result in far fewer total deaths than generally predicted, e.g. 500k were predicted for the UK without measures (ICL, March 2020).
All of our actions (lockdowns etc) have been based on the beliefs that everyone is susceptible to infection; that only a small percentage have been infected so far, &; that the virus could kill some 0.5~1% of the population (e.g. 500k UK deaths with no measures, ICL March 2020).
Reason & evidence (this discussion being but one example of many) would suggest that this is not the case & that we may well have overestimated the overall risk by a factor of about 10.

[Analysis, thoughts, opinions & errors my own]
_Note re data:_
ONS classify any mention of Covid on a death certificate as Covid death & take no account of testing issues. True Covid deaths are therefore debatable, especially in recent months, but we can use these data to compare regions.
ONS classify any mention of Covid on a death certificate as Covid death & take no account of testing issues. True Covid deaths are therefore debatable, especially in recent months, but we can use these data to compare regions.
_Note re normalisation of data:_
Charts here are normalised by year to date non-Covid deaths. i.e. Covid deaths relative to normal mortality. This, whilst not perfect, is more useful for comparisons.
Charts here are normalised by year to date non-Covid deaths. i.e. Covid deaths relative to normal mortality. This, whilst not perfect, is more useful for comparisons.
• • •
Missing some Tweet in this thread? You can try to
force a refresh







