1/17
How does calcium "stabilize the cardiac membrane" in hyperkalemia?
I learned early in my intern year to use calcium in the setting of severe hyperkalemia.
I never really learned how it works. The answer requires some history. And uncovers a forgotten alternative treatment.
How does calcium "stabilize the cardiac membrane" in hyperkalemia?
I learned early in my intern year to use calcium in the setting of severe hyperkalemia.
I never really learned how it works. The answer requires some history. And uncovers a forgotten alternative treatment.

2/
First, some history.
While Sidney Ringer was developing his eponymous fluid, he observed that increasing potassium content led to progressively weaker ventricular contractions.
He reported these findings in 1883.
pubmed.ncbi.nlm.nih.gov/16991336/
First, some history.
While Sidney Ringer was developing his eponymous fluid, he observed that increasing potassium content led to progressively weaker ventricular contractions.
He reported these findings in 1883.
pubmed.ncbi.nlm.nih.gov/16991336/

3/
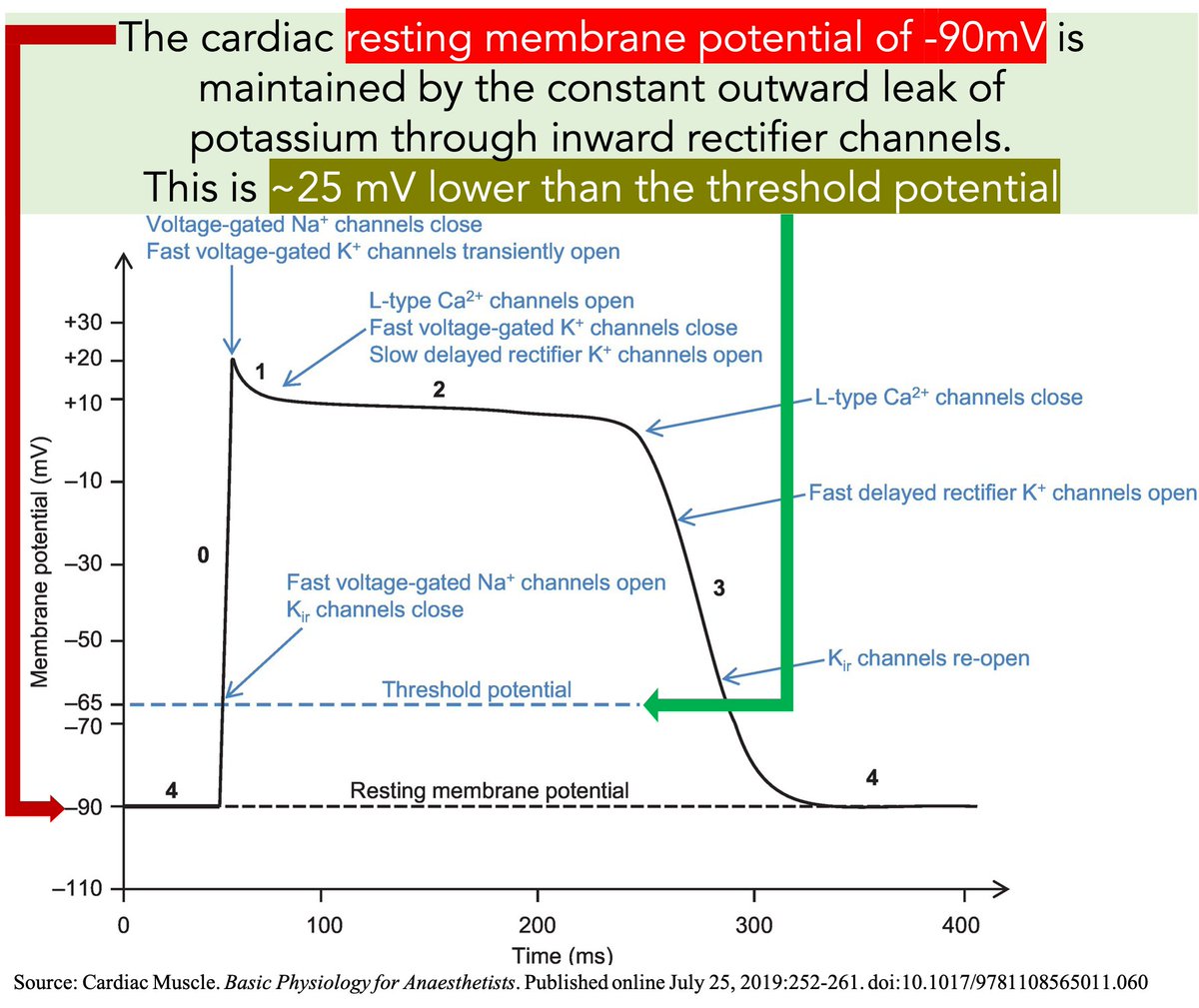
How does hyperkalemia affect the heart? To understand the answer, recall that the generation of an action potential is dependent on the:
(1) resting membrane potential (−90mV for myocytes)
(2) threshold potential (-70mV)
(3) activation state of membrane sodium channels
How does hyperkalemia affect the heart? To understand the answer, recall that the generation of an action potential is dependent on the:
(1) resting membrane potential (−90mV for myocytes)
(2) threshold potential (-70mV)
(3) activation state of membrane sodium channels

4/
And also recall that the resting membrane potential results from the outward leak of potassium.
This leak of positively charged ions leaves the inner membrane relatively negative.
pathophys.org/physiology-of-…
And also recall that the resting membrane potential results from the outward leak of potassium.
This leak of positively charged ions leaves the inner membrane relatively negative.
pathophys.org/physiology-of-…
5/
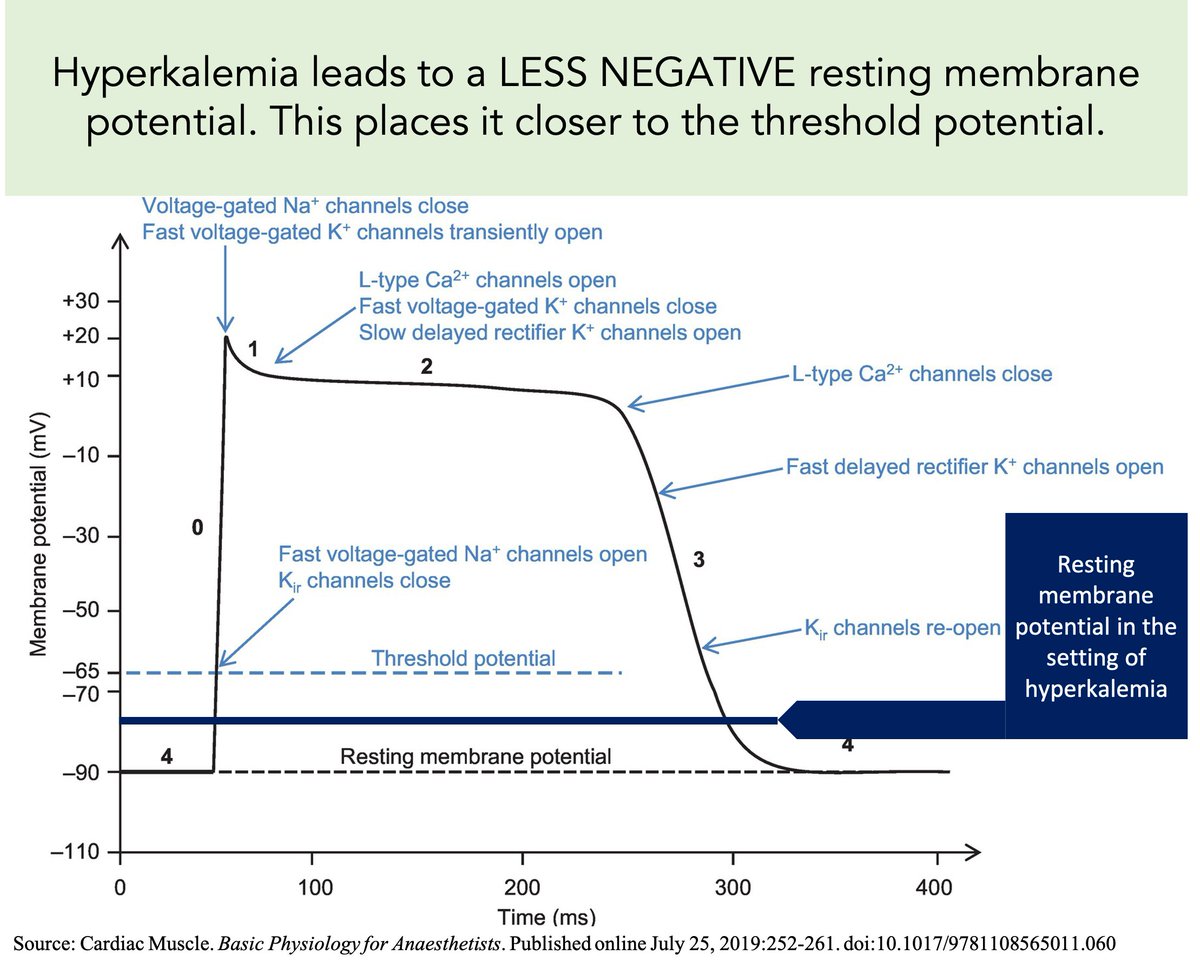
🔑As the serum potassium increases, the gradient for outward flow diminishes. This leaves the resting potential LESS negative...
...and closer to the threshold potential.
Result: 💥Increased myocyte excitability💥
You might even say it is "unstable".
🔑As the serum potassium increases, the gradient for outward flow diminishes. This leaves the resting potential LESS negative...
...and closer to the threshold potential.
Result: 💥Increased myocyte excitability💥
You might even say it is "unstable".
6/
How does calcium "stabilize" this unstable (excitable) membrane? There are at least two options:
(1) Decrease the resting potential (i.e., make it MORE negative)
(2) Increase the threshold potential (i.e., move it further away from the resting potential)
Which is it?
How does calcium "stabilize" this unstable (excitable) membrane? There are at least two options:
(1) Decrease the resting potential (i.e., make it MORE negative)
(2) Increase the threshold potential (i.e., move it further away from the resting potential)
Which is it?
7/
In 1955 Silvio Weidmann showed that MORE depolarization was required in calcium-rich solutions.
🔑The resting potential was unchanged, but the threshold potential had INCREASED.
He concluded that "this accounts for the 'stabilizing' effect of Ca."
pubmed.ncbi.nlm.nih.gov/13264118/
In 1955 Silvio Weidmann showed that MORE depolarization was required in calcium-rich solutions.
🔑The resting potential was unchanged, but the threshold potential had INCREASED.
He concluded that "this accounts for the 'stabilizing' effect of Ca."
pubmed.ncbi.nlm.nih.gov/13264118/

8/
Interim Summary
➢ Hyperkalemia increases the resting potential, bringing it closer to the threshold potential
➢ This makes myocytes excitable/unstable
➢ Calcium increases the threshold potential, moving it further from the resting potential, stabilizing the myocyte membrane
Interim Summary
➢ Hyperkalemia increases the resting potential, bringing it closer to the threshold potential
➢ This makes myocytes excitable/unstable
➢ Calcium increases the threshold potential, moving it further from the resting potential, stabilizing the myocyte membrane
9/
Again, hyperkalemia increases the resting potential leading to INCREASED membrane excitability.
But...
...a persistent increase in resting potential inactivates sodium channels required for Phase 0. This leads to DECREASED membrane excitability.
pubmed.ncbi.nlm.nih.gov/1190336/
Again, hyperkalemia increases the resting potential leading to INCREASED membrane excitability.
But...
...a persistent increase in resting potential inactivates sodium channels required for Phase 0. This leads to DECREASED membrane excitability.
pubmed.ncbi.nlm.nih.gov/1190336/
10/
The decrease in membrane excitability is shown by a decreased rate of rise (Vmax) of phase 0 of the action potential.
Why is Vmax slower?
🔑The resting potential during depolarization determines the number of active sodium channels.
pubmed.ncbi.nlm.nih.gov/16572868/
The decrease in membrane excitability is shown by a decreased rate of rise (Vmax) of phase 0 of the action potential.
Why is Vmax slower?
🔑The resting potential during depolarization determines the number of active sodium channels.
pubmed.ncbi.nlm.nih.gov/16572868/

11/
At -90 mV (the normal resting potential), the maximum number of channels are open.
As the resting potential increases (as with hyperkalemia), fewer channels are open leading to slower depolarization (i.e., decreased Vmax).
pubmed.ncbi.nlm.nih.gov/16572868/
At -90 mV (the normal resting potential), the maximum number of channels are open.
As the resting potential increases (as with hyperkalemia), fewer channels are open leading to slower depolarization (i.e., decreased Vmax).
pubmed.ncbi.nlm.nih.gov/16572868/

12/
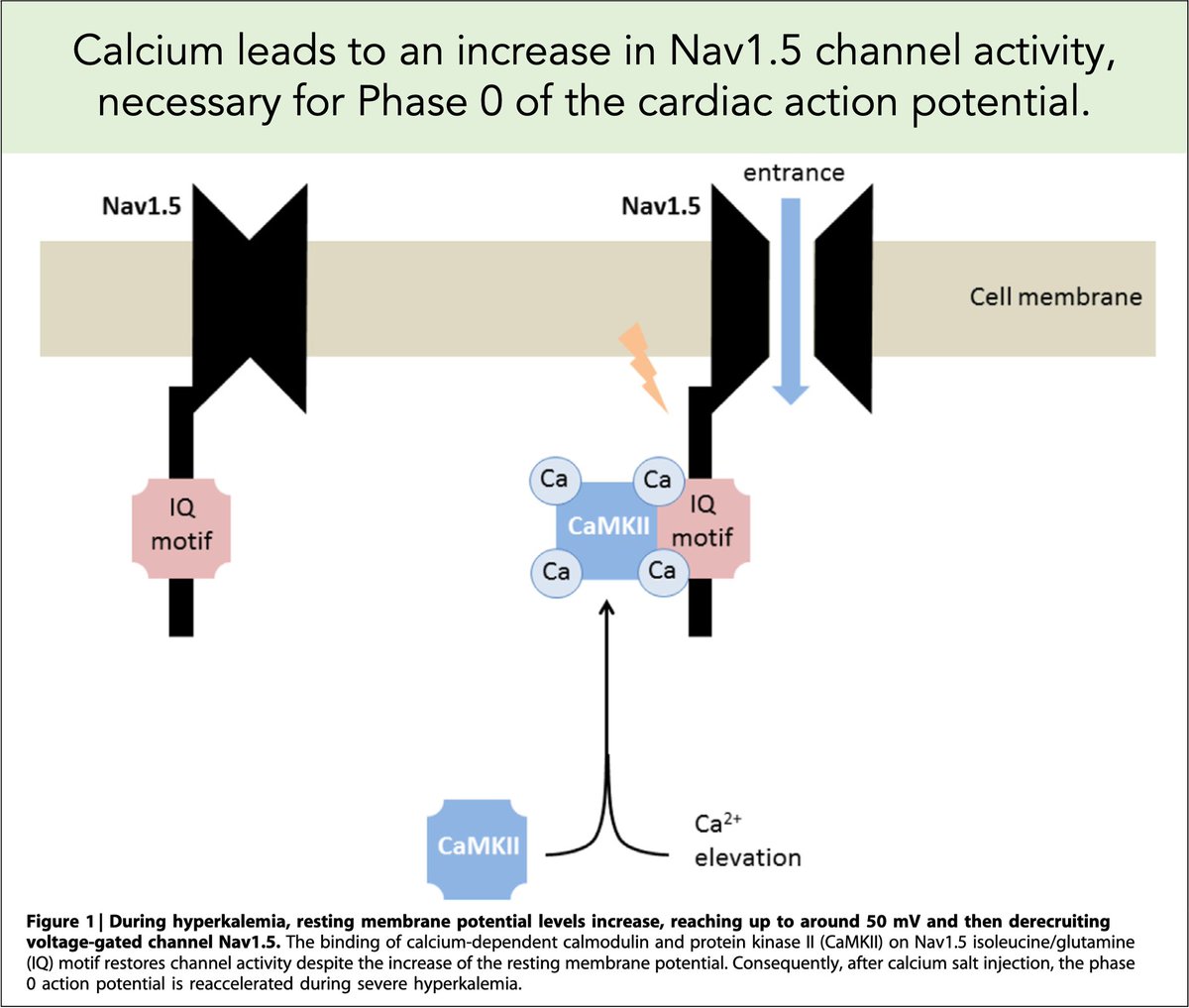
To protect against this second mechanism, any intervention must mitigate the inactivation of sodium channels.
Calcium does this!
It increases the activity of Nav 1.5 sodium channels required for Phase 0 depolarization.
pubmed.ncbi.nlm.nih.gov/27418095/
To protect against this second mechanism, any intervention must mitigate the inactivation of sodium channels.
Calcium does this!
It increases the activity of Nav 1.5 sodium channels required for Phase 0 depolarization.
pubmed.ncbi.nlm.nih.gov/27418095/
13/
Another treatment has been shown to mitigate the effects of hyperkalemia.
Since at least 1918, hypertonic saline has been shown effective at combatting the cardiotoxic effects of hyperkalemia.
I had never heard of this as a treatment.
jpet.aspetjournals.org/content/12/1/19
Another treatment has been shown to mitigate the effects of hyperkalemia.
Since at least 1918, hypertonic saline has been shown effective at combatting the cardiotoxic effects of hyperkalemia.
I had never heard of this as a treatment.
jpet.aspetjournals.org/content/12/1/19

14/
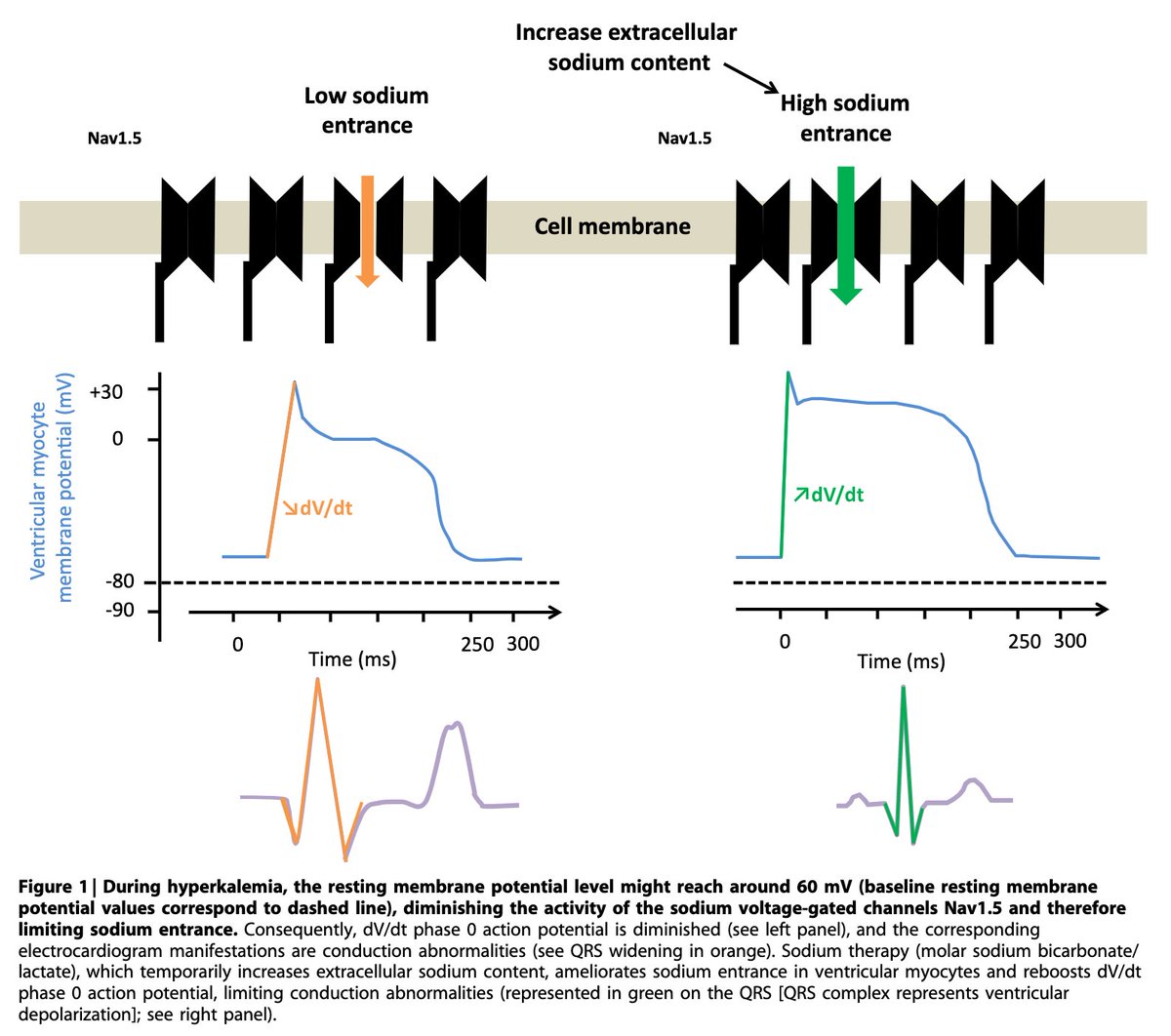
Just as with calcium, hypertonic saline can increase Vmax via activation of Nav 1.5 sodium channels.
Simplistically, the increased extracellular sodium concentration increases the velocity of flow across the cell membrane when the channels open.
pubmed.ncbi.nlm.nih.gov/27418094/
Just as with calcium, hypertonic saline can increase Vmax via activation of Nav 1.5 sodium channels.
Simplistically, the increased extracellular sodium concentration increases the velocity of flow across the cell membrane when the channels open.
pubmed.ncbi.nlm.nih.gov/27418094/
15/
Hypertonic saline can have similar effects to those seen with calcium.
For example, you can see improvement in the ECG abnormalities caused by hyperkalemia. So cool!
pubmed.ncbi.nlm.nih.gov/13896850/
Hypertonic saline can have similar effects to those seen with calcium.
For example, you can see improvement in the ECG abnormalities caused by hyperkalemia. So cool!
pubmed.ncbi.nlm.nih.gov/13896850/

16/
Before closing, an observation: in reviewing the literature, I am surprised how easily calcium became the standard of care. Before the 1970s, saline and calcium were vying for primacy!
To read more, see my post on The Curious Clinicians site.
curiousclinicians.com/a-brief-histor…
Before closing, an observation: in reviewing the literature, I am surprised how easily calcium became the standard of care. Before the 1970s, saline and calcium were vying for primacy!
To read more, see my post on The Curious Clinicians site.
curiousclinicians.com/a-brief-histor…
17/17
➢ Initially, hyperkalemia increases the resting potential making myocytes MORE excitable
➢ The increased resting potential inactivates sodium making myocytes LESS excitable
➢ Calcium salts address both of these issues
➢ Hypertonic saline may also be beneficial
➢ Initially, hyperkalemia increases the resting potential making myocytes MORE excitable
➢ The increased resting potential inactivates sodium making myocytes LESS excitable
➢ Calcium salts address both of these issues
➢ Hypertonic saline may also be beneficial
• • •
Missing some Tweet in this thread? You can try to
force a refresh