Yesterday the world lost a shining light, much too soon. @marjoriesue’s life was marked by tragedy – widowed early with two young children, then metastatic cancer – but she radiated joy and empathy and was an astonishingly gifted writer. In memoriam, some of my favorite pieces: 

Margi was a pediatrician, writer, friend, researcher and community activist, but also a single mom who raised two extraordinary young women. Here, she wrote nicer words about other people's mothers (including mine @renalis) than I have ever said to my own:
wbur.org/cognoscenti/20…
wbur.org/cognoscenti/20…
On dating while on chemo
nytimes.com/2020/09/04/sty…
nytimes.com/2020/09/04/sty…
On baby birds and empty nests
cnn.com/2019/08/22/opi…
cnn.com/2019/08/22/opi…
On getting bad news instead of giving bad news
nytimes.com/2020/03/13/wel…
nytimes.com/2020/03/13/wel…
On how to truthfully remember a deceased loved one, set in the context of a (different) plague; this one is especially poignant to re-read right now
tabletmag.com/sections/commu…
tabletmag.com/sections/commu…
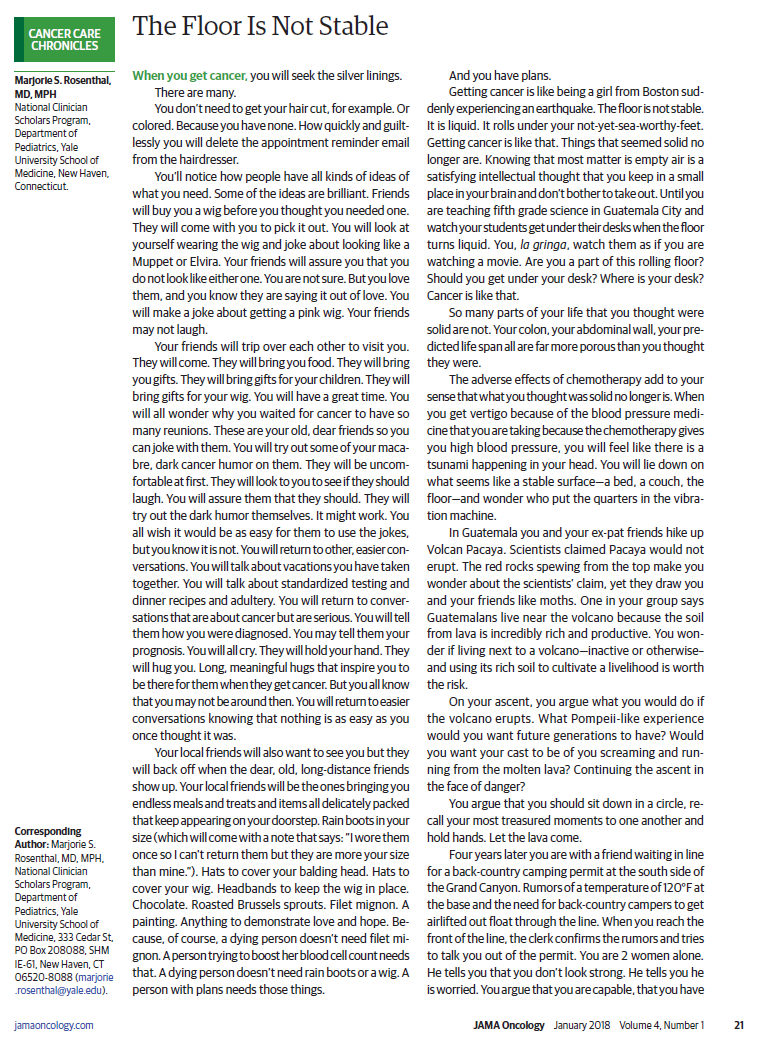
On adapting to a cancer diagnosis pubmed.ncbi.nlm.nih.gov/28973150/

On connecting at a distance
nytimes.com/2020/05/05/wel…
nytimes.com/2020/05/05/wel…
On why parenting (and quality improvement) is like my favorite movie medium.com/@marjorie.rose…
On relating differently to patients as a single parent pubmed.ncbi.nlm.nih.gov/16820535/


On the misguided push to encourage patients to shame doctors and nurses into washing their hands
wbur.org/commonhealth/2…
wbur.org/commonhealth/2…
In her writing, fairly bursting with a deep love and compassion for others, she leaves an indelible gift to her daughters, family, friends and countless strangers: a deeply personal record of who she really was.
I wish you all had had the privilege of knowing her in person. But I know her writing will make her memory a blessing for many beyond her many friends. @muffysart @lesliecyale @joshmoejo @lfiellin @thehowie @nicoleFluhr @hkgn @EmilyMelnick7 @JsscHlhn



• • •
Missing some Tweet in this thread? You can try to
force a refresh