
We set out to identify the sensitivity & specificity of common tests for #COVID19 along w/ @dan_diekema , @Anthony98947615 w/ @CDCgov support
A simple enough task, right?
I’ve seen tweets by @DrSidMukherjee @drjohnm @BenMazer @PaulSaxMD @BradSpellberg and others interested
1/n
A simple enough task, right?
I’ve seen tweets by @DrSidMukherjee @drjohnm @BenMazer @PaulSaxMD @BradSpellberg and others interested
1/n
Looking for comments/criticism
What are we missing? No industry adverts please!
Important papers?
2/n
What are we missing? No industry adverts please!
Important papers?
2/n
The @US_FDA has a test comparison site that is incomprehensible to me… but @ASMicrobiology types tell me it reports on analytical sensitivity and LoD for tests
3/n
3/n
First, terms:
As a clinician, I want to know if a patient does or doesn’t have #covid19.
I’m less concerned by internal laboratory QA unless it translates
We wanted what has been called CLINICAL or diagnostic sensitivity/ specificity NOT analytical sen/sp.
4/n
As a clinician, I want to know if a patient does or doesn’t have #covid19.
I’m less concerned by internal laboratory QA unless it translates
We wanted what has been called CLINICAL or diagnostic sensitivity/ specificity NOT analytical sen/sp.
4/n
Described in 1997:
Clinical “diagnostic sensitivity is defined by the percentage of persons who have the disorder of interest who have positive results on the assay”
And more recently early in COVID by @akesselheim
nejm.org/doi/full/10.10…
5/n
Clinical “diagnostic sensitivity is defined by the percentage of persons who have the disorder of interest who have positive results on the assay”
And more recently early in COVID by @akesselheim
nejm.org/doi/full/10.10…
5/n

Another note, PCR has largely been the laboratory gold standard.
So, most reports are for sen/sp relative to PCR—not to a clinical gold standard.
We adjusted reported results to reflect:
e.g. PCR Sen 90% x Antigen Sen of 50% = overall antigen Sen of 45%
6/n
So, most reports are for sen/sp relative to PCR—not to a clinical gold standard.
We adjusted reported results to reflect:
e.g. PCR Sen 90% x Antigen Sen of 50% = overall antigen Sen of 45%
6/n
Finally, we are NOT talking about being infectious for #covid19.
That is another topic with even LESS data I hope to share soon.
Suffice to say, many people with #COVID19 disease are NOT infectious, especially after a week or 10 days, but some tests still +, esp PCR
7/n
That is another topic with even LESS data I hope to share soon.
Suffice to say, many people with #COVID19 disease are NOT infectious, especially after a week or 10 days, but some tests still +, esp PCR
7/n
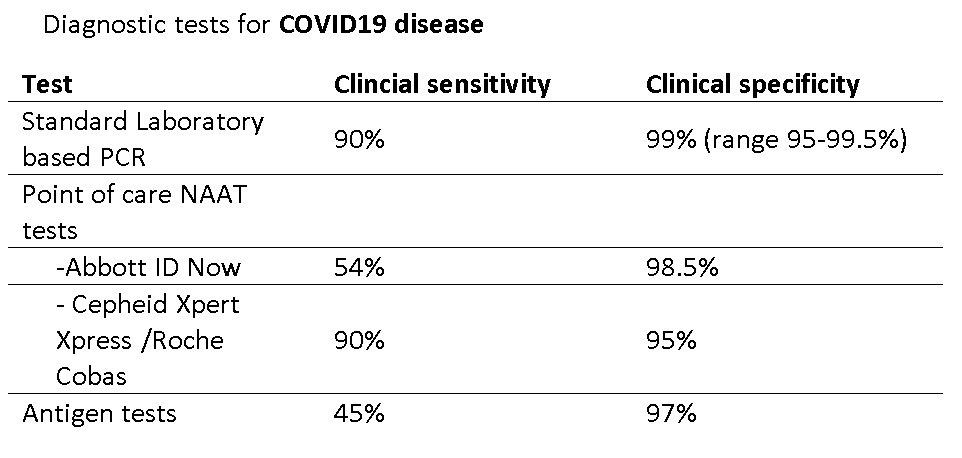
PCR—the gold standard
Clinical sensitivity ~ 90% on day 4 of symptoms w/ common instruments
sciencedirect.com/science/articl…
dx.plos.org/10.1371/journa…
jcm.asm.org/content/58/8/e…
academic.oup.com/ofid/article-a…
8/n
Clinical sensitivity ~ 90% on day 4 of symptoms w/ common instruments
sciencedirect.com/science/articl…
dx.plos.org/10.1371/journa…
jcm.asm.org/content/58/8/e…
academic.oup.com/ofid/article-a…
8/n
-earlier reports of lower PCR sensitivity had atypical gold standard or were not reporting optimal sampling on day 4
-Sensitivity IS lower before/ after day 4 of symptoms per acpjournals.org/doi/10.7326/M2…
9/n
-Sensitivity IS lower before/ after day 4 of symptoms per acpjournals.org/doi/10.7326/M2…
9/n
Reasons for PCR false-negatives (10% false – rate)
lack of virus in sampling site
inadequate sampling
lack of instrument optimization or variation between instruments
10/n
lack of virus in sampling site
inadequate sampling
lack of instrument optimization or variation between instruments
10/n
PCR Clinical Specificity ~99%
this was hard!
Scant data, authors suggest between 95%-99.5%
bmj.com/content/369/bm…
gov.uk/government/pub…
cdc.gov/csels/dls/locs…
m.koreaherald.com/view.php?ud=20…
jcm.asm.org/content/58/8/e…
11/n
this was hard!
Scant data, authors suggest between 95%-99.5%
bmj.com/content/369/bm…
gov.uk/government/pub…
cdc.gov/csels/dls/locs…
m.koreaherald.com/view.php?ud=20…
jcm.asm.org/content/58/8/e…
11/n
Reasons for PCR false-positives (~1% false + rate)
-past infection with residual RNA
-differences in testing between instruments
-glitches in instrument reading of Ct/Cq values
-lack of laboratory optimization normally required by the FDA
-contamination
12/n
-past infection with residual RNA
-differences in testing between instruments
-glitches in instrument reading of Ct/Cq values
-lack of laboratory optimization normally required by the FDA
-contamination
12/n
Next, the Point of Care NAAT tests
Limited information published and in some ways very similar to lab based PCR
Abbott IDNow seems less sensitivity/more specific than Cepheid Xpert Xpress/Roche Cobas
13/n
Limited information published and in some ways very similar to lab based PCR
Abbott IDNow seems less sensitivity/more specific than Cepheid Xpert Xpress/Roche Cobas
13/n
POC NAAT tests
—Abbott IDNow
Clinical Sensitivity 54% / Clinical specificity 97.5%
(final numbers after adjustment for comparison to PCR)
Misses high CT value PCR + which are often NON-infectious. But no data vs. cell culture
cochranelibrary.com/cdsr/doi/10.10…
amazing work @deeksj
14/n
—Abbott IDNow
Clinical Sensitivity 54% / Clinical specificity 97.5%
(final numbers after adjustment for comparison to PCR)
Misses high CT value PCR + which are often NON-infectious. But no data vs. cell culture
cochranelibrary.com/cdsr/doi/10.10…
amazing work @deeksj
14/n
other POC NAAT sources
jcm.asm.org/content/58/8/e…
jcm.asm.org/content/58/8/e…
ncbi.nlm.nih.gov/pmc/articles/P…
sciencedirect.com/science/articl…
15/n
jcm.asm.org/content/58/8/e…
jcm.asm.org/content/58/8/e…
ncbi.nlm.nih.gov/pmc/articles/P…
sciencedirect.com/science/articl…
15/n
We estimated
Cepheid Xpert Xpress /Roche
Overall
Clinical sensitivity 90%
Clinical Specificity 95%
jcm.asm.org/content/58/8/e…
pubmed.ncbi.nlm.nih.gov/32417674/
(and other refs for IDNow)
16/n
Cepheid Xpert Xpress /Roche
Overall
Clinical sensitivity 90%
Clinical Specificity 95%
jcm.asm.org/content/58/8/e…
pubmed.ncbi.nlm.nih.gov/32417674/
(and other refs for IDNow)
16/n
Last, but not least...
Antigen tests! The great promise.
I would say useful but not great.
Overall
Clinical sensitivity 45%
Clinical specificity 97%
cochranelibrary.com/cdsr/doi/10.10…
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
17/n
Antigen tests! The great promise.
I would say useful but not great.
Overall
Clinical sensitivity 45%
Clinical specificity 97%
cochranelibrary.com/cdsr/doi/10.10…
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
17/n
False +s with Antigen tests are real
cleveland.com/coronavirus/20…
dpbh.nv.gov/uploadedFiles/…
ahcancal.org/Data-and-Resea…
18/n
cleveland.com/coronavirus/20…
dpbh.nv.gov/uploadedFiles/…
ahcancal.org/Data-and-Resea…
18/n
Antigen tests better detect live virus but VERY limited data vs. cell culture @michaelmina_lab
And newer antigen tests will likely be better (but need clinical data, not just lab comparisons)
19/n
And newer antigen tests will likely be better (but need clinical data, not just lab comparisons)
19/n
So, in conclusion, a group of @IDSAInfo docs, epidemiologists and @ASMicrobiology estimated the following CLINICAL Sensitivity & specificity for #COVID19 diagnostic tests
--feedback welcome
--feedback welcome
• • •
Missing some Tweet in this thread? You can try to
force a refresh


