As @hankgreen nicely points out, we have to be careful that "we don't know whether the vaccine reduces transmission" doesn't morph into "the vaccine doesn't reduce transmission." How do we communicate this uncertainty? A few thoughts. 1/7
https://twitter.com/hankgreen/status/1341165997294637056
First, vaccine efficacy against infection can't be higher than vaccine efficacy against disease. If something prevents infection, it also prevents disease. But vaccines can work by preventing symptoms, and so give an extra boost to efficacy against disease. 2/7
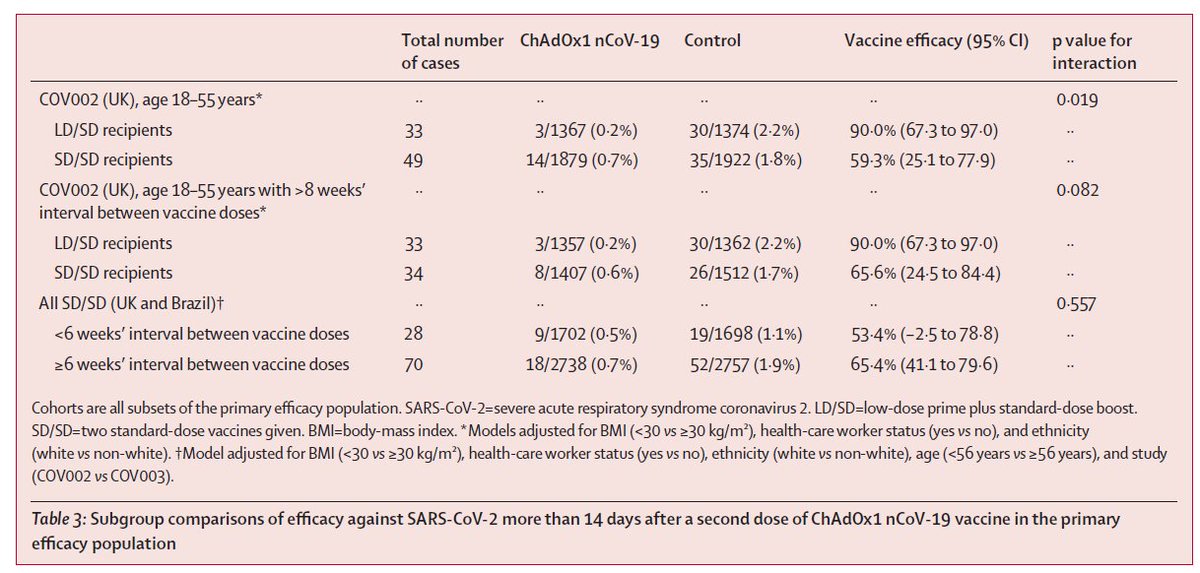
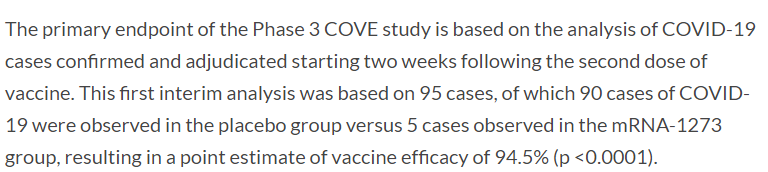
So while we expect vaccine efficacy against infection to be lower, we aren't sure how much. We have a bit of data from the UK/Oxford and Moderna trials showing reduced infection, but we are waiting on antibody testing data from these and other trials. 3/7
https://twitter.com/megtirrell/status/1338831902636208129?s=20
Even if the vaccines have lower efficacy against infection, meaning vaccinated people still get infected, there are other ways for vaccines to provide indirect protection. They could reduce the duration or amount of viral shedding, making people less infectious. 4/7
Relatedly, we have accruing evidence that people who never experience symptoms are less contagious than people who do. So maybe if a vaccine works well enough to prevent symptoms, it could also make these people less contagious? 5/7
nature.com/articles/d4158…
nature.com/articles/d4158…
The above is more complex to sort out. We can use viral shedding data, but this is generally only available from symptomatic trial participants. We could also conduct specialized tracing studies or cluster randomized trials, but this takes time. 6/7
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
But for now, the way I frame it is:
- With 95% efficacy against disease, it seems likely that the vaccine is providing some level of indirect protection.
- We have to make policy decisions now, despite uncertainty, so we try to balance what we know with what we expect. 7/7
- With 95% efficacy against disease, it seems likely that the vaccine is providing some level of indirect protection.
- We have to make policy decisions now, despite uncertainty, so we try to balance what we know with what we expect. 7/7
• • •
Missing some Tweet in this thread? You can try to
force a refresh