Short THREAD.
On False POSITIVES of rapid antigen tests.
This 🧵 is on SPECIFICITY or the issues of False POSITIVES and rapid antigen tests.
Many people are concerned that these fast, inexpensive tests cause too many false positives and will overload PCR labs...
1/x
On False POSITIVES of rapid antigen tests.
This 🧵 is on SPECIFICITY or the issues of False POSITIVES and rapid antigen tests.
Many people are concerned that these fast, inexpensive tests cause too many false positives and will overload PCR labs...
1/x
Rapid antigen tests can have 98%-99.9% specificity meaning between 0.1% and 2% of tests run might be falsely positive.
If prevalence is low, even a 99.9% specificity could mean many of the positive tests are falsely positive.
But w rapid tests, there are rapid solutions!
2/x
If prevalence is low, even a 99.9% specificity could mean many of the positive tests are falsely positive.
But w rapid tests, there are rapid solutions!
2/x
Many ppl instinctively worry that a false positive will mean an erroneous 10 day isolation and that huge numbers of people are going to require laboratory based PCR confirmation tests and this will overload the system.
No, this is stuck-in-our-ways thinking...
3/x
No, this is stuck-in-our-ways thinking...
3/x
With rapid tests, we don’t have to send in a PCR test for confirmation - it’s much simpler than that in a “rapid test world” - we can use a second rapid test... right there and have a confirmatory result in moments.
We do this all the time with HIV tests...
4/x
We do this all the time with HIV tests...
4/x
With HIV tests, if prevalence is low, ~50% of our positives may be false positive.
We don’t say the test is useless. We don’t make the person wait a week for a new test. We simply run the test on a second similar also imperfect test - combined they are very accurate.
5/x
We don’t say the test is useless. We don’t make the person wait a week for a new test. We simply run the test on a second similar also imperfect test - combined they are very accurate.
5/x
W Rapid Ag tests, we can simply repeat the exact same test a second time. That will get rid of most false positives in five minutes.
Alternatively we just use two different rapid antigen tests. Every house has 10 yellow tests and 2 red confirmatory rapid tests...
6/x
Alternatively we just use two different rapid antigen tests. Every house has 10 yellow tests and 2 red confirmatory rapid tests...
6/x
If you turn positive on yellow test, use the red one. They look same but have different molecules. Will not be expected to turn falsely positive for the same reason.
This can get false positives to <1:2000 or, one false positive every few years if testing 2x /week.
7/x
This can get false positives to <1:2000 or, one false positive every few years if testing 2x /week.
7/x
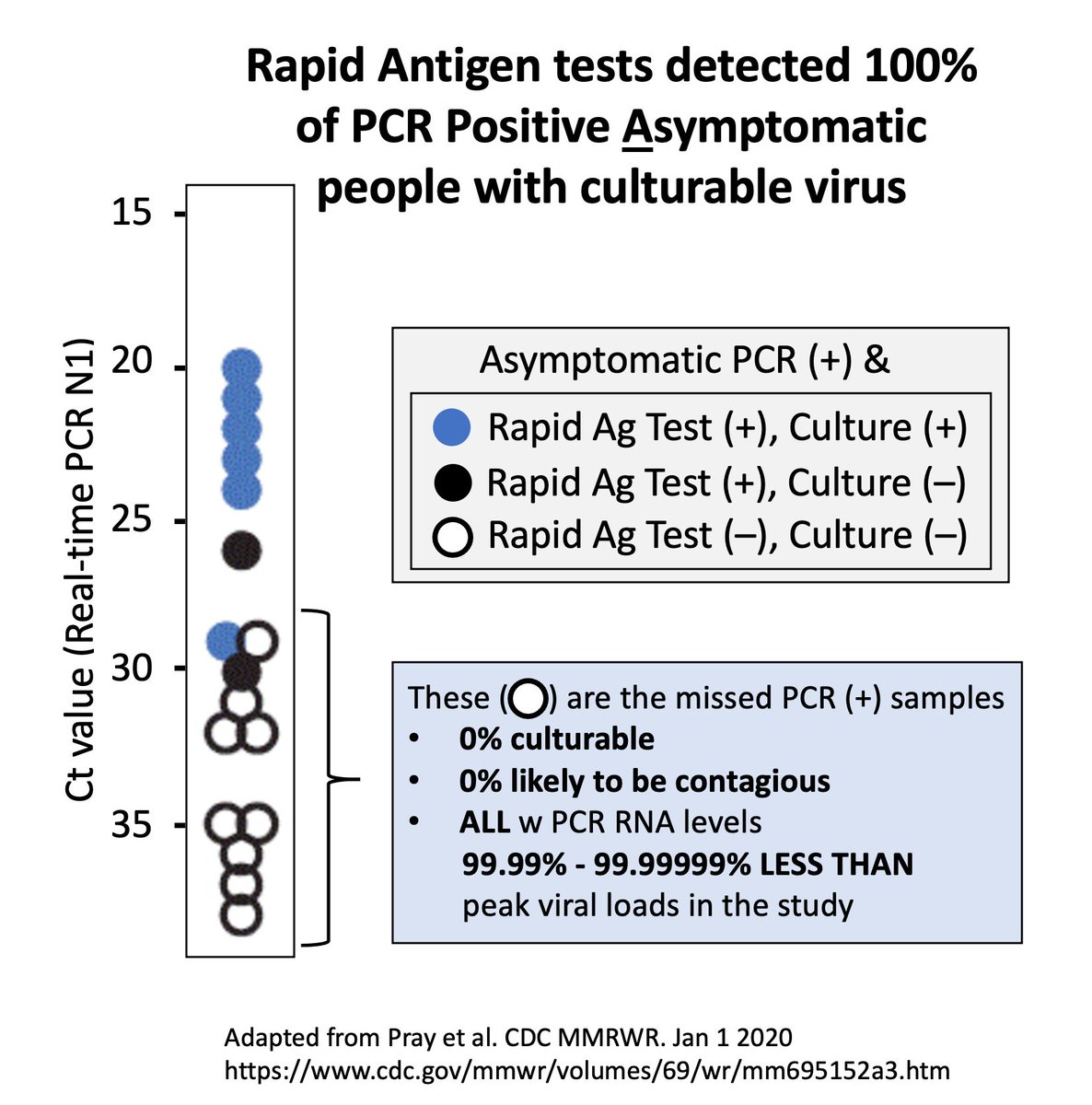
In this same @CDCMMWR paper I’ve discussed, the authors found that each time they retested what turned out to be a false positive again w the exact same test, the test turned negative.
Within minutes ppl can know a positive is true or false.
cdc.gov/mmwr/volumes/6…
8/x
Within minutes ppl can know a positive is true or false.
cdc.gov/mmwr/volumes/6…
8/x
Therefore, we do not need need PCR tests and instead a massive rapid test program will ease the burden on PCR labs, NOT increase it.
We just have to take a step back and recognize there are simple solutions here.
Also - we can keep testing, hours later, or next day
9/x
We just have to take a step back and recognize there are simple solutions here.
Also - we can keep testing, hours later, or next day
9/x
The repeated convenient testing that rapid antigen tests afford not only GREATLY improve sensitivity over PCR (discussed elsewhere), but importantly increase specificity as well.
A false positive doesn’t mean automatic 10 day isolation when you can confirm at will.
10/x
A false positive doesn’t mean automatic 10 day isolation when you can confirm at will.
10/x
That type of thinking is what happens when we only focus on lab based, slow, expensive Clinical diagnostic tests. For mass population screening, we have so many more options w rapid tests to improve sensitivity, specificity and massively improve EFFECTIVENESS of testing.
11/11
11/11
Also, last point - with a two test approach - we need to stop calling a single positive that doesn’t repeat, false.
We should consider the duo of tests as married. In that @CDCMMWR study above, they called them false positives even though they confirmed within minutes
12/x
We should consider the duo of tests as married. In that @CDCMMWR study above, they called them false positives even though they confirmed within minutes
12/x
Ideally, we should look at it as a testing algorithm. If both tests turn out to be the rare 2x false positive - THEN call it a false positive. Otherwise call it as it is - screening plus confirmation. We measure the program as the primary endpoint, not the individual parts.
13/x
13/x
If you’ve gotten this far an you are asking “but what about false negatives - I thought those are the major concern” yes. This was simply a thread about false positives.
I’ve written extensively about concern over false negatives as well.
Here’s one thread about it
I’ve written extensively about concern over false negatives as well.
Here’s one thread about it
https://twitter.com/michaelmina_lab/status/1345911598414786561
• • •
Missing some Tweet in this thread? You can try to
force a refresh