1/ Covid Chronicles, Day 307
One of the most challenging parts of Covid has been grappling with decision-making under uncertainty. It’s natural for MDs to weigh risks & benefits; med school trained us in probabilistic decision-making. But it’s an unnatural act for most people.
One of the most challenging parts of Covid has been grappling with decision-making under uncertainty. It’s natural for MDs to weigh risks & benefits; med school trained us in probabilistic decision-making. But it’s an unnatural act for most people.
2/ And it's even harder w/ Covid. Just as you’ve gotten comfortable with a situation – Should I go to the store? Have a drink outside w/ friends? – the numbers change.
So let’s take a few minutes to go through some math – the kind of math you need to make rational choices.
So let’s take a few minutes to go through some math – the kind of math you need to make rational choices.
3/ Let’s start w/ a basic tenet of decision-making in Covid: there is nothing that's perfectly safe, & nothing that's totally risky. Everything is about probabilities. What do I mean? A good cloth mask isn’t 100% effective, but it does lower chances of getting infected by 70-80%.
4/ An N95 is even better (~90-95%). Staying 6 feet away from people is awfully safe, but not 100% – 10 feet would be safer. All of us have learned these things (& others: outdoors better than in, ventilation better than not) over the past year, & we’ve all developed a set of…
5/ … things we will and won’t do.
But just as you grown confident w/ these choices, conditions change – and so do the probabilities... and, sometimes, the optimal choice of activities. In this thread, I’ll tackle a few of these changes, focusing on three: 1) changing local…
But just as you grown confident w/ these choices, conditions change – and so do the probabilities... and, sometimes, the optimal choice of activities. In this thread, I’ll tackle a few of these changes, focusing on three: 1) changing local…
6/ …prevalence rates; 2) vaccines; & 3) mutants. Let’s start with changing local prevalence rates. Here, the key takeaway is that the chance of being infected from a given encounter is the product of the risk level of the encounter (ie, mask wearing or not, inside vs. outside)…
7/ … multiplied by the probability that the person you came into contact with has Covid & is infectious. This second part leads to some tricky decision making. For example, “Is it safe to be 6 feet away from someone, inside, both wearing masks?” is hard to answer w/o knowing…
8/ … the probability that the person has Covid. And that's hard to be certain of without knowing whether they're sick (raises the probability), had a recent negative test (lowers it, though not to zero), & has been behaving safely (impossible to know). And remember, going from…
9/ …being near 1 person to 4 raises chance of transmission a lot. This is all nicely shown by my fave “How Risky Is a Given Activity?” calculator: @microcovid. Plugging in this scenario (in SF, inside, 15 minutes, 1 other person, masks, 6ft apart), it shows a transmission risk…
10/ …of ~1/17,000. Same encounter in LA (⬆ prevalence) is riskier: 1 in 5,000. Group of 4 people instead of 1 (in LA): up to 1 in 1,428. Change the conditions, change the probabilities.
(BTW, @WIRED piece on origin of @microcovid by six SF housemates: tinyurl.com/y4kr7of3)
(BTW, @WIRED piece on origin of @microcovid by six SF housemates: tinyurl.com/y4kr7of3)
11/ (Interestingly, @microcovid just made a very conservative assumption: all estimates now based on assumption that UK variant will become the dominant strain in the U.S. That may happen, but it hasn’t happened yet.)
The UK variant (B117) seems to be ~50% more infectious…
The UK variant (B117) seems to be ~50% more infectious…
12/ …than the old SARS-CoV-2 we’ve been battling. In the U.S., do we need to change activity in response to this threat? I asked @angie_rasmussen & Paul Turner this @inthebubblepod; both recommended we “double down” on old precautions, not add new ones.
tinyurl.com/yywbdrd3
tinyurl.com/yywbdrd3
13/ So while you may not need to act MORE safely than before, ~50% more transmissible means that – if you’ve been cheating a bit – an activity you got away with in 2020 might fail you now. So doubling down seems like the minimum – personally, I would up my safety game a smidge.
14/ Here’s more math (& where I think @microcovid was too conservative): currently, the UK variant makes up only a small fraction of U.S. cases. (Yes, I know we haven’t looked very hard and it’s undoubtedly more prevalent than we appreciate. But still I don't know any expert…
15/ …who believes that the UK variant makes up >10% of virus in any U.S. community, at least not yet.) So, in thinking about the risk of the UK variant, one shouldn't (yet) factor in a high prevalence. Back of the envelope calc: a 50% more infectious virus that makes up ~10%…
16/ …of cases in a community should lead you to act 5% more safely – a rounding error. So in U.S., Angie’s/Paul’s double-down advice seems sound: continue to act safely & don’t let down your guard. This would change if the variant takes off, as it might (and it did in England).
17/ The impact of vaccines is also complicated. Let’s say you’ve sorted out your acceptable activities based on your pre-vaccinated state. Should that change post-vaccine? Here, you have to understand the timeline of protection; shown here for the Pfizer vaccine (the one I got). 
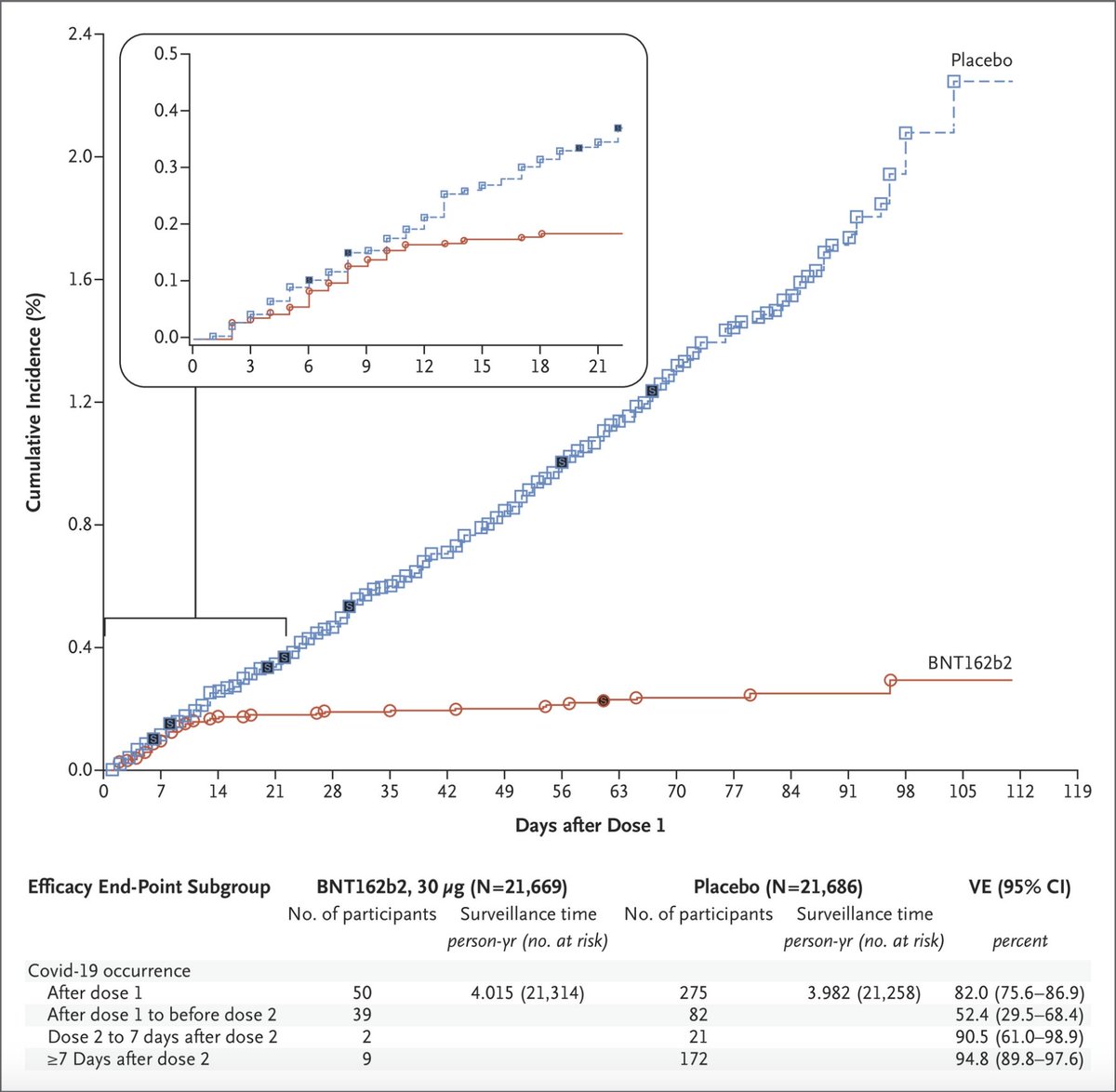
18/ Protection starts ~10d after shot one, when you’re ~50% protected. So hypothetically, if you were in a region where all the virus was UK variant (50% more infectious) & you were 10 days post-shot #1 (50% protected), you’d be back to ~normal risk (with old virus & no vaccine).
19/ Back to vaccine: would you change behavior at 50% protected? I didn’t. When I went to work in the hospital I still wore 2 masks. But I did feel a bit less anxious, which is worth something! Just before my 2nd shot, Pfizer curve showed I was ~80-90% protected, which still…
20/ …wasn’t enough to cause me to change activities.
Now I’m 1 week after shot #2, so I should be ~95% protected. Note that this means that I can still get Covid (w/ millions vaccinated, it’s not surprising that we’re hearing about a few post-vaccine cases – 95% isn’t 100%)…
Now I’m 1 week after shot #2, so I should be ~95% protected. Note that this means that I can still get Covid (w/ millions vaccinated, it’s not surprising that we’re hearing about a few post-vaccine cases – 95% isn’t 100%)…
21/ …but it’s darn close to complete protection, particularly since Pfizer & Moderna studies found no cases of severe Covid (needing hospitalization, ICU, or leading to death), vs. ~40 in the placebo group.
What will I do now? I won’t ditch my mask, at least not until the…
What will I do now? I won’t ditch my mask, at least not until the…
22/ …science shows I’m not capable of catching Covid & spreading it. (Here’s a nice thread by @awgaffney on what we do/don’t know re: vaccination & transmission – we DO know that it will decrease transmission; we just don’t know by how much tinyurl.com/y4vzld85).
23/ Even with 95% protection, I’ll still be a bit concerned about catching Covid if I’m in a high-risk situation or a place w/ a sky-high prevalence. But I WILL do 3 things I haven’t done in 6 months: get a real haircut, see a dentist, & fly to see my son in GA & parents in FL.
24/ This is complex stuff; here’s how I process it: think about your baseline risk w/ “classic” Covid (& activities you were comfy doing). Then ⬆risk if there’s a local surge; ⬆ risk if high prevalence of more infectious variant; & ⬇ risk based on degree of vaccine protection.
25/ Of course in assessing overall risk, you need to multiply risk of getting Covid by risk you’ll get sick & die (influenced by age & co-morbidities).
I know it’s a lot to process; but this is the drill until we hit herd immunity, when we can just live our lives. Can't wait!
I know it’s a lot to process; but this is the drill until we hit herd immunity, when we can just live our lives. Can't wait!
• • •
Missing some Tweet in this thread? You can try to
force a refresh