As expected, our @washingtonpost editorial today on the delayed second dose vaccine strategy has generated a vigorous and interesting dialogue. tinyurl.com/y7c6v9hz Here are my takeaways (a thread): 1/18
The debate is healthy. There are pros and cons to the current strategy and the alternative we present, and there are real uncertainties associated with them both. They should debated thoughtful and studied to the degree possible. 2/18
Many people seem focused on the source of the delays in vaccination, as if it matters whether the bottleneck is from vaccine production or distribution/injection. I don’t think it does. Starting soon, there will be doses available and people to inject them – and... 3/18
... the next dose can either go to someone who is coming around for their second injection 3-4 weeks after their first, or to someone getting their first shot. Policymakers need to choose which strategy does the most good at a societal level. 4/18
As we said in the op-ed, it may make sense to stick with the early 2nd dose to the most vulnerable (over 75, nursing home) or most exposed (frontline healthcare workers). The small drop in efficacy from the 2nd-dose-later strategy might be quite meaningful in these groups. 5/18
Nothing about our stance should imply that we shouldn’t be doing everything possible to improve supply & distribution – as if it's one or the other. This is a public health emergency – we must move faster.
But even more focus & funding won't fix the problems quickly... 6/18
But even more focus & funding won't fix the problems quickly... 6/18
... and so the question remains: what to do when we have a dose that is ready to be injected. Particularly with the threat of the new, more contagious variant looming. 7/18
Some have called sticking w/ the timing used in the trials “scientific” & altering the timing "not scientific". To me, this is polemical. The studies may not have been primarily focused on testing the question of how effective the 1st dose is before giving the 2nd dose...8/18
... But they DID test it, within the limits of statistical inference. "Scientific" is not just a clinical trial, but also the sciences of public policy, public health, epidemiology, & sociology. We have to take all the information we have and use it to make the best choices. 9/18
In terms of the counter-arguments that have been raised today, few credible scientists have argued that a 2 month delay in dose 2 will compromise the strength/durability of the ultimate immune response. In fact, some have argued that it might enhance it. 10/18
The possibility that immunity will wane between doses 1 and 2 has been raised by some, but also doesn’t seem to be a major concern – particularly given the miniscule reinfection rate that we’ve seen from natural infection and the robust immune response seen after dose one. 11/18
The most credible arguments – and I know @ashishkjha and I are both concerned about them – are:
a. The possibility that “partial immunity” will spawn harmful mutations – we'll need more virologists to weigh in on this; it could change the calculus tinyurl.com/y9f6xlrm 12/18
a. The possibility that “partial immunity” will spawn harmful mutations – we'll need more virologists to weigh in on this; it could change the calculus tinyurl.com/y9f6xlrm 12/18
b. Concern that delay means more people won’t return for 2nd dose – we can probably estimate this from other programs w/ return visits at variable times. Is it really true that people will have a harder time coming back in 3 months than 1, or we'll lose track of them more? 13/18
c. Whether change in vaccine schedule will lead to more vaccine hesitancy. I could see this going either way – delayed 2nd dose gives more people a chance at earlier vaccination during a surge, so could increase rates. Or the opposite, from another curveball. Hard to know. 14/18
Choosing to change to the deferred 2nd dose strategy is is a big decision (note that the UK has already made it) and so we need our best experts thinking about it. We should also be looking at sophisticated models that use credible inputs for all the key variables:... 15/18
... including efficacy after 1 vs. 2 doses, impact of delay on efficacy & durability of immunity, reasonable estimates of missed second dose and overall vaccination rates, estimated frequency and impact of clinically meaningful mutations. But most importantly... 16/18
... overall lives saved, and lost, with each potential strategy.
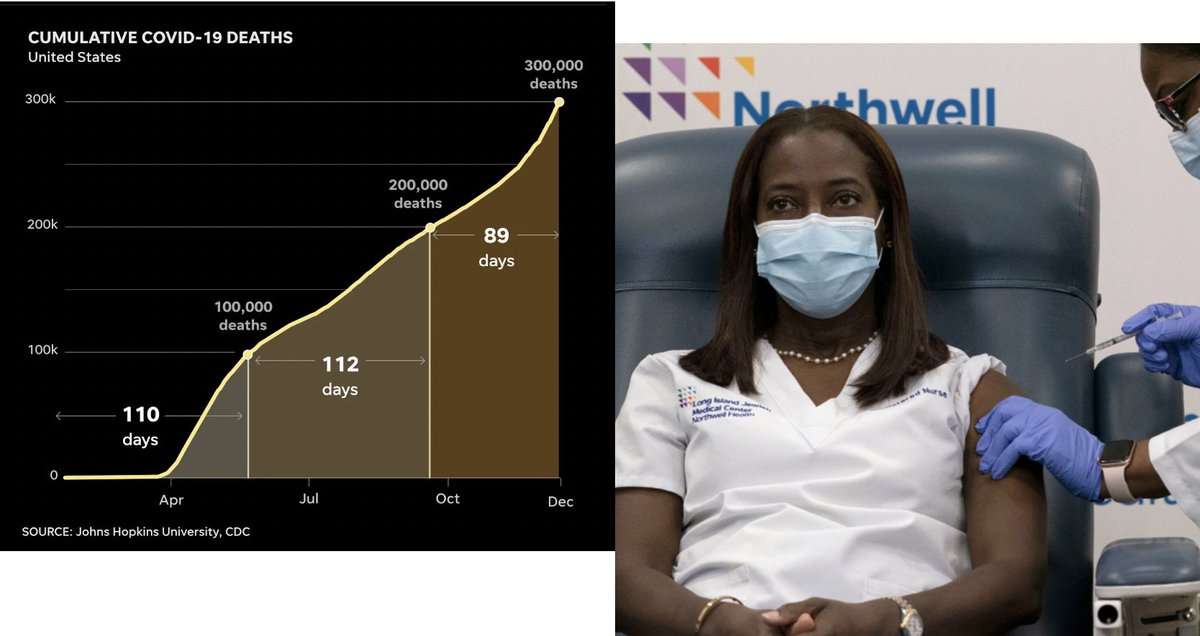
The context for the debate is the near certainty that we'll lose another 50-100K Americans this month, and we're threatened by a mutation that may accelerate the tragedies. So time is a crucial variable. 17/18
The context for the debate is the near certainty that we'll lose another 50-100K Americans this month, and we're threatened by a mutation that may accelerate the tragedies. So time is a crucial variable. 17/18
Our goal was to contribute to the debate, and it has mostly been civil & fact-based. Everybody wants to take advantage of these amazingly effective vaccines to save the most lives. Let’s put our best minds, data, and models to this question, so we can make the best choices. 18/18
• • •
Missing some Tweet in this thread? You can try to
force a refresh