Please don't panic too much about these new variants of SARS-CoV-2. Taking a step back, RNA viruses (viruses that use RNA as their genetic material rather than DNA; SARS-CoV is an RNA virus) have higher mutation rates than DNA viruses (like chickenpox).
jvi.asm.org/content/92/14/…
jvi.asm.org/content/92/14/…
Their RNA-dependent RNA polymerases (which replicate the genetic material) do not "proofread" assiduously like DNA polymerases so random mutations occur and those that confer a "fitness advantage" (helps them replicate more efficiently) take off. See this:
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
Mutations that lead to an enhancement of the ability of the spike protein to bind to the host's receptor (the ACE receptor) may be advantageous to the virus. Of 295,507 full-length genome sequences of SARS-CoV-2 worldwide, authors looked at mutations affecting that interface and
found a handful affecting that interface. But vaccines (all of them to date - Moderna; Pfizer; AZ) have genetic material that code for the entire spike protein & the RBD (receptor binding protein) and generate multiple antibodies to that region, even though papers show us only 2
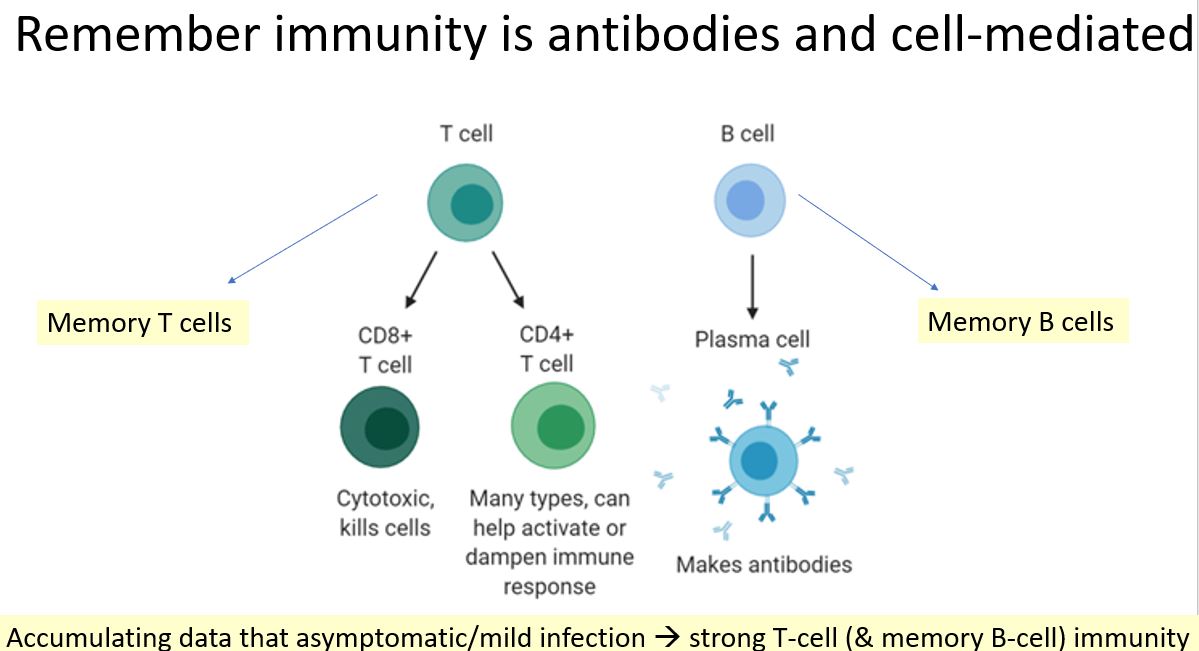
So, with the generation of multiple antibodies (not all measured in the papers), B cell and T cell response, immunity to the variants with vaccines should be retained. And "tweaks' can be made to the genetic material in future if needed in vaccines to boost response even more
• • •
Missing some Tweet in this thread? You can try to
force a refresh