
Know very tempting to feel nervous about variants. Please don't: 1) RNA viruses do mutate and those more fit spread more readily; 2) SARS-CoV-2 has much lower mutational rate than influenza A - we are seeing more because transmission high, want to tamp down (& now sequencing);
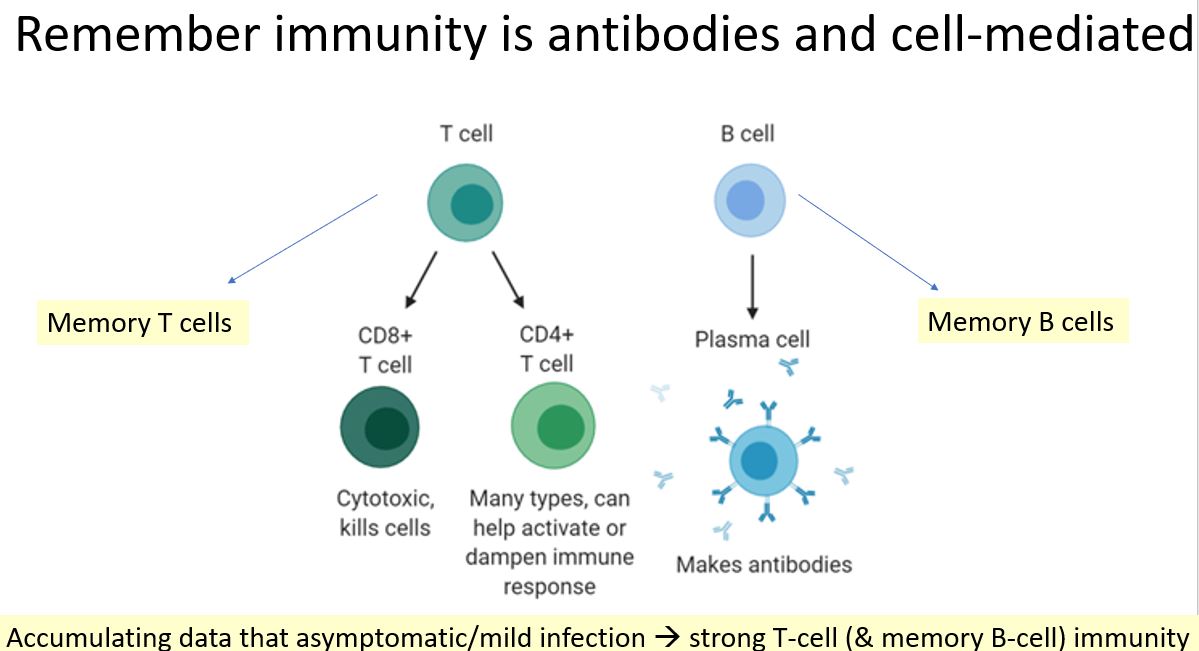
3) Vaccines do not generate just antibody response, but T cell responses (measured in all 3 trials published) and B cell responses). So if neutralizing antibodies slightly lower in vaccinated blood to a variant (and not yet lower in clinically significant way), remember T cells. 
4) So far, all of these vaccines involve genetic material that code for the spike protein/RBD- mRNA in mRNA vaccines and double-stranded DNA in adenovector vaccines. Sequences of genetic material can be "tweaked" to respond to variants as needed; 5) As tweeted before, efficacy
of all of these vaccines great for such a prevalent (and world-halting) virus; 6) The fact that severe disease prevented 100% by all of these vaccines means they really tamp down viral load which likely related to severity- they work against this virus super well.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


