At risk of upsetting people, I need to address why I think teachers should feel very safe going to in-person learning after vaccination. Let's start with why COVID-19 was a bad virus and how vaccines defang this virus and then let me address transmission one more time. As said
many times, Moderna and Pfizer phase 3 trials were meant to assess the risk of COVID-19 infection with symptoms as they were designed for expediency. So, 1st outcome was 1) do you have any symptoms suggestive of COVID-19, we will swab and see if you have COVID-19? 2nd outcome was
did you get severe disease from COVID-19?. In terms of 1st outcome to look at, 95% of COVID-19 cases with symptoms occurred in people who got placebo, not vaccine. Vaccine massively reduced chance of getting COVID-19 with symptoms. In 2nd outcome, all of the severe COVID-19
cases that occurred across both trials happened in those who got placebo; vaccine seemed to protect from the most severe outcomes 100% (please see former tweets for breakdown and the 1 case in Pfizer marked "severe" but not). So a teacher who is fully vaccinated will be protected
from what they fear most- symptomatic COVID-19 and severe disease (no matter who they are around, children or adults). Okay, now let's address transmission again without controversy. What that means is can you still have SARS-CoV-2 in your nose if you have been vaccinated? e.g.
asymptomatically carry it? The trials were not designed to answer that question but Pfizer/Moderna will be answering that question with post-vaccination swabs of vaccinated individuals -please see answers to CDC here:
leadingage.org/regulation/cdc…
leadingage.org/regulation/cdc…
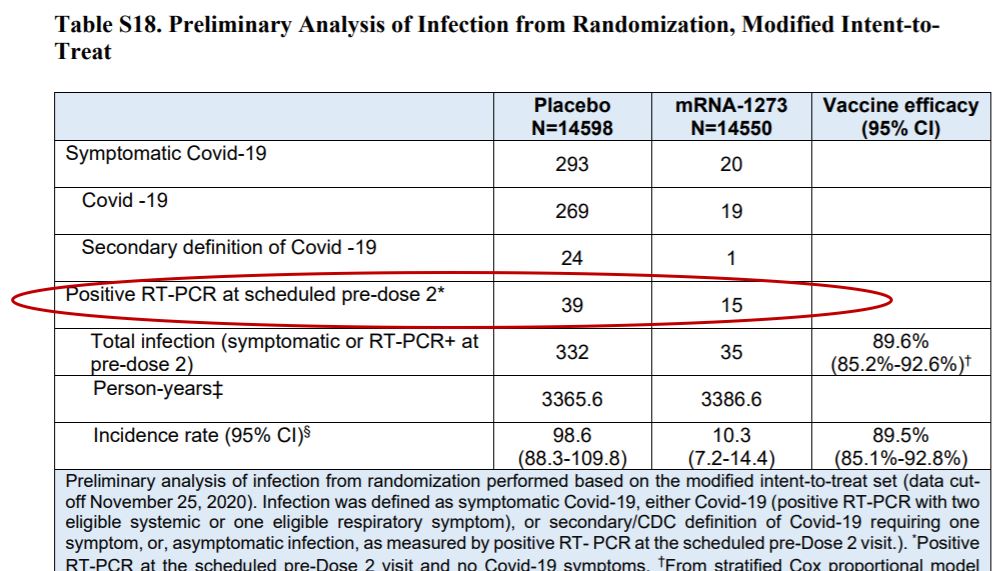
Is there some suggestive data that the vaccines will reduce asymptomatic carriage? Pfizer did not look at that question at all in interim phase 3 trial results published in NEJM. Moderna's phase 3 trial design actually did swab before the 2nd dose (without regard to symptoms) so
could assess asymptomatic carriage then and below is the figure from their table (look at supplement) & attached is the paper. There is a 62% risk reduction in having asymptomatic carriage in your nose with getting 1 dose of Moderna vaccine versus placebo:
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
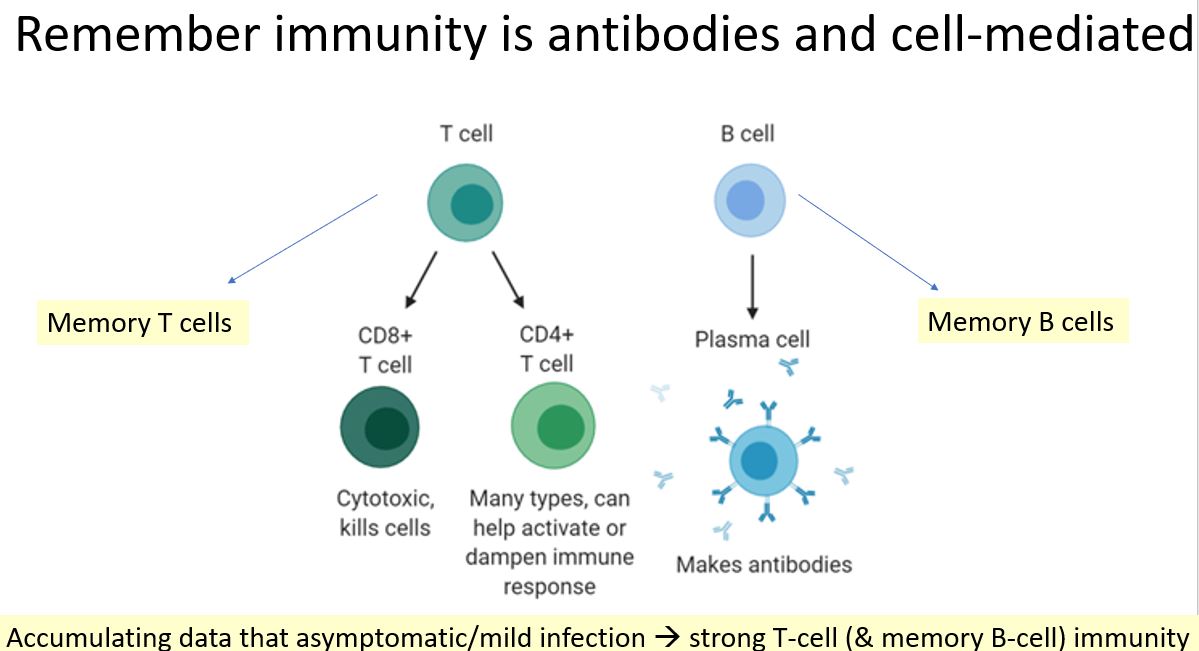
Then you ask- well, if mRNA vaccines stimulate IgG (antibodies measured in trials), T cell and B cell immunity as documented- is there a reason to think that IgG could also help block virus at the mucosal (nose) surface (since IgA is the "immunoglobulin" or antibody that
predominantly mediates mucosal immunity?). Yes, biologic reason to believe serum IgG would help block infection at mucosal surfaces as well- this has been shown with other viruses- some examples here (serum IgG helps block rotavirus):
pnas.org/content/102/20…
pnas.org/content/102/20…
And IgG (the antibodies measured in those trials) are found in high quantities at mucosal surfaces. Please see this review:
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
So, even though we wait those further studies from Pfizer/Moderna (and independent groups, UCSF group putting in grant too) on regular swabbing after vaccines and the recommendation is that vaccinated should mask/distance to protect unvaccinated for now, biological plausibility
of reducing asymptomatic carriage. Finally, back to teachers: even if exposed to virus, they have the vaccination which has rendered the virus toothless so they are safe. I know most teachers are interested in returning which is why teachers were put in Tier 1B for early vax
I hope this paper gets added to the thread about parenteral vaccination also inducing IgA immunity (that is antibody type in mucosal surfaces like noses!)
cvi.asm.org/content/23/6/4…
cvi.asm.org/content/23/6/4…
And the Moderna and Pfizer vaccines neutralize even global variants ("UK" and "South Africa") so don't worry there!
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
Here is the Pfizer data on not significant reduction in efficacy against the UK and South Africa variants. We are good here!
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
• • •
Missing some Tweet in this thread? You can try to
force a refresh