#MedTwitter -- it is time for another new #MedEd Model!
This #Tweetorial is the first in a series (#CurricDevMEM) and is made with support from the incredible @Doc_JD_!
This #Tweetorial is the first in a series (#CurricDevMEM) and is made with support from the incredible @Doc_JD_!

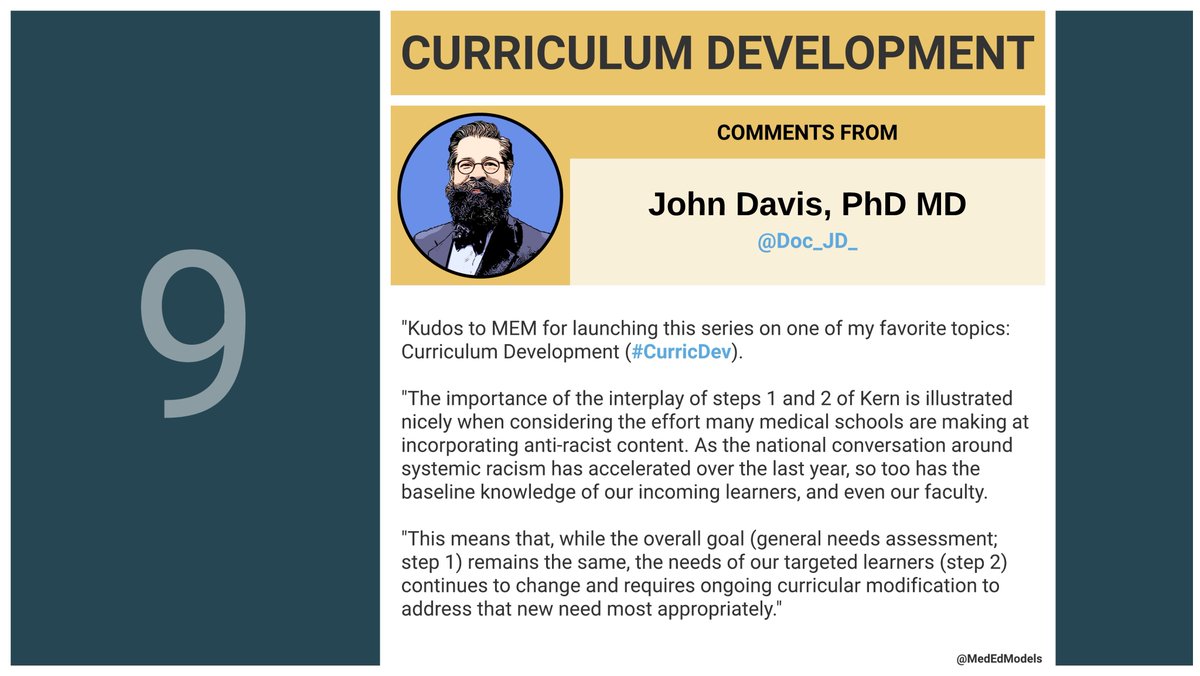
We will explain the first two steps of Kern's approach to curricular development and describe strategies for completing a problem identification, general needs assessment, & targeted needs assessment.

Curricular development has 6 steps.
Check out the image below for a visual summary of these steps & how they connect in the process of curriculum development.
Check out the image below for a visual summary of these steps & how they connect in the process of curriculum development.

Of Kern’s 6 Steps for curricular development, we’ll focus on #1 & 2 today.
Since problem identification & general needs assessment each deserve attention, we’ve split step 1 into two parts - see the image for details!
Since problem identification & general needs assessment each deserve attention, we’ve split step 1 into two parts - see the image for details!

Let’s start w/ the problem identification.
The goal is to identify a healthcare related problem that has an impact on society.
Starting at the societal level helps us ensure we select a relevant problem. From there, we can work to understand the factors that contribute to it.
The goal is to identify a healthcare related problem that has an impact on society.
Starting at the societal level helps us ensure we select a relevant problem. From there, we can work to understand the factors that contribute to it.

Once we have a relevant & well-defined problem, a general needs assessment (GNA) helps us understand where the gaps are.
GNA can focus on education or be more comprehensive (what are patients, healthcare providers, society doing?). For this #MEM, we focused on education!
GNA can focus on education or be more comprehensive (what are patients, healthcare providers, society doing?). For this #MEM, we focused on education!

Now, you’re ready to determine your project type. We made an algorithm to help, #MedTwitter!
What was the result of your last problem ID & general needs assessment? Reply below!
What was the result of your last problem ID & general needs assessment? Reply below!

It can feel deflating as an education scholar to find yourself at outcome 1.
However, this is also a great opportunity to build an interprofessional team for your education project!
However, this is also a great opportunity to build an interprofessional team for your education project!
Reaching across boundaries and working with clinical or social science researchers to understand the problem can catalyze rich collaboration in health professions education.
After your general needs assessment, you can start to focus on the specific learners you’ll work with in your targeted needs assessment.
We’d love you hear from you #MedTwitter!
What have you found helpful in conducting targeted needs assessments? Reply below and let us know.
We’d love you hear from you #MedTwitter!
What have you found helpful in conducting targeted needs assessments? Reply below and let us know.

We’ve been a bit conceptual up to this point, so let’s get specific.
See the image below for a worked example of STEP 1 & 2!
It’s dense, but we promise it’s worth it ;)
See the image below for a worked example of STEP 1 & 2!
It’s dense, but we promise it’s worth it ;)

For this #MEM, our prompt is a *big* question: in the modern age, what should be core content in med school?
This study from @AcadMedJournal is a great example of one attempt to define core ().
Check out the image & reply with your own ideas, #MedTwitter! bit.ly/36oY4Kx
This study from @AcadMedJournal is a great example of one attempt to define core ().
Check out the image & reply with your own ideas, #MedTwitter! bit.ly/36oY4Kx

We’re super lucky for this #MEM to have thoughts from @Doc_JD_, including ideas about defining core content for medical school.
Thank you for participating, John!
Thank you for participating, John!
Here’s the bottom line. Let us know what you learned!
How will this affect your approach to curricular projects in #MedEd?
How will this affect your approach to curricular projects in #MedEd?

#MEM is a primer - let us set you up To Learn More (#2LM)!
Check out these scholars' work:
@Doc_JD_
@JenniferDeitz4
@DrMayaAdam
@PaulPottingerMD
@PCH_SF
@BSchwartzinSF
@Sherilyn_Smith
@arianneteherani
Particularly in:
@MedEduc_Journal
@AcadMedJournal
@MedEdPortal
@AAMCtoday
Check out these scholars' work:
@Doc_JD_
@JenniferDeitz4
@DrMayaAdam
@PaulPottingerMD
@PCH_SF
@BSchwartzinSF
@Sherilyn_Smith
@arianneteherani
Particularly in:
@MedEduc_Journal
@AcadMedJournal
@MedEdPortal
@AAMCtoday

Long overdue, but this extremely popular #MedEdModel is now available in a text-only format
docs.google.com/document/d/13m…
docs.google.com/document/d/13m…
• • •
Missing some Tweet in this thread? You can try to
force a refresh