Announcing: brief report for Fall 2020 intervention surveillance @GeorgiaTech represents the work of many, released to help inform, guide, and improve efforts to use viral testing as part of integrative mitigation.
A thread follows...
medrxiv.org/content/10.110…
A thread follows...
medrxiv.org/content/10.110…

Key messages:
Viral testing can mitigate outbreaks, when used at scale.
Expect outbreaks to be heterogeneous (both 'good' and 'bad' news with respect to control).
Passive testing is not enough, we recommend using infectious data to reinforce testing/control.
...
Viral testing can mitigate outbreaks, when used at scale.
Expect outbreaks to be heterogeneous (both 'good' and 'bad' news with respect to control).
Passive testing is not enough, we recommend using infectious data to reinforce testing/control.
...
Key metapoint: models helped inform the scale and frequency of testing, but the point of intervention was not to score theoretical points (e.g., post-hoc matching of models and data don't help stop cases here and now).
...
...
Instead, it is critical to develop cognitively simple approaches to response, enabling individual decision-makers to react intuitively and rapidly (i.e., develop instruments but let humans fly).
For example: reinforce testing/quarantine/contact tracing in incipient clusters.
For example: reinforce testing/quarantine/contact tracing in incipient clusters.
Point 1: Viral testing can mitigate outbreaks, when used at scale.
Take-away for policymakers, more testing implies more documented cases in the near term but fewer actual cases in the long-term.
Take-away for policymakers, more testing implies more documented cases in the near term but fewer actual cases in the long-term.
Soon after Fall 2020 term, a case cluster was identified in a Greek house, and then more cases in other Greek houses and adjacent residences. Rather than view such events passively, we responded by increasing testing, messaging, and contact tracing.
Hence, although we found many cases, the process of identifying cases and/or quarantining individuals came early enough that we rapidly went from 4% positivity to <1% (compared to UGA which saw post-entry rates approach 9%).

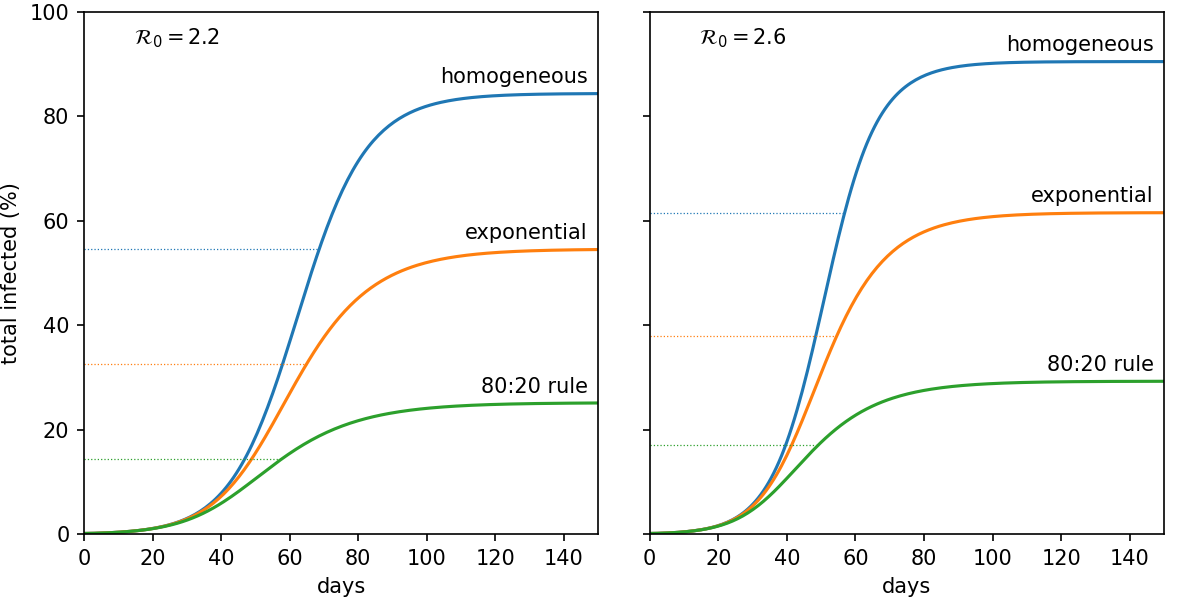
Point 2. Expect outbreaks to be heterogeneous.
As was documented in multiple town halls in the Fall, we observed a 75-25 rule (i.e., subset of houses/halls with disproportionate share of cases), e.g.,:
figshare.com/articles/prese…
As was documented in multiple town halls in the Fall, we observed a 75-25 rule (i.e., subset of houses/halls with disproportionate share of cases), e.g.,:
figshare.com/articles/prese…

This is challenging, because we would have been hard pressed to predict the 'seed' cluster in advance. But, once identified, the clustering of cases means that targeted responses can be more effective than in a 'homogeneous' mixing model where transmission is equal everywhere.
Hence, the bad news of large localized outbreaks can be 'good' news, if one works to use testing to identify locales and reinforce mitigation efforts.
Point 3. Passive testing is not enough, we recommend using infectious data to reinforce testing.
This does not get enough attention in models, policy, or press. Testing must be a form of active response.
This does not get enough attention in models, policy, or press. Testing must be a form of active response.
My advice to colleges/firms starting to return to work w/testing plans: look at the data... every night and use as a guide to adjust responses. Don't try and score theoretical points, try to make a practical difference.
To do so, keep in mind that under-testing usually implies that a few cases are the tip of a cluster-berg. Formally speaking this is contained in hypergeometric distributions (but even using simple guidelines of connected spread are enough to initiate reinforcement testing).
Message out to localized halls/houses (or floors), with an expectation of testing a few days after identification of case cluster. Hence, when testing becomes active, you can learn from information and help mitigate.
In August 2020, GT re-opened in a difficult context (elevated spread in Georgia and the South, generally), because of work that had started months on the lab, logistics, and analytics side.
We continue to see ~1% positivity, continue to provide free, fast, and simple saliva-based testing and aim for transparency in reporting cases.
And one last point: testing is key, but is not a panacea.
One of the precursors that made this possible, was a summer effort by many to make sure that masks were required on campus.
ajc.com/blog/get-schoo…
One of the precursors that made this possible, was a summer effort by many to make sure that masks were required on campus.
ajc.com/blog/get-schoo…
That early win set the stage for an integrated approach, because the benefits of less intensive testing (we have capacity for weekly testing) increases w/NPIs.

Full details of the report available via @medrxivpreprint , and deeply grateful to work of @genomestake, Michael Shannon, JulieAnne Williamson and dozens of others who made (and continue to make) this intervention possible.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…

p.s. Editors interested in seeing this in a journal, feel free to ping (seriously), at present the #Covid19 publication review process is broken in many ways, so delighted to engage to reduce wasted time/effort and find a good fit to vet results and enhance sharing w/community.
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh