We've updated our preprint on the transmissibility of SARS-CoV-2 VOC 202012/01, aka B.1.1.7, with new statistical and modelling methods. Headline: we estimate VOC is 43–82% more transmissible than preexisting variants. UNDER PEER REVIEW cmmid.github.io/topics/covid19… (1/6) 

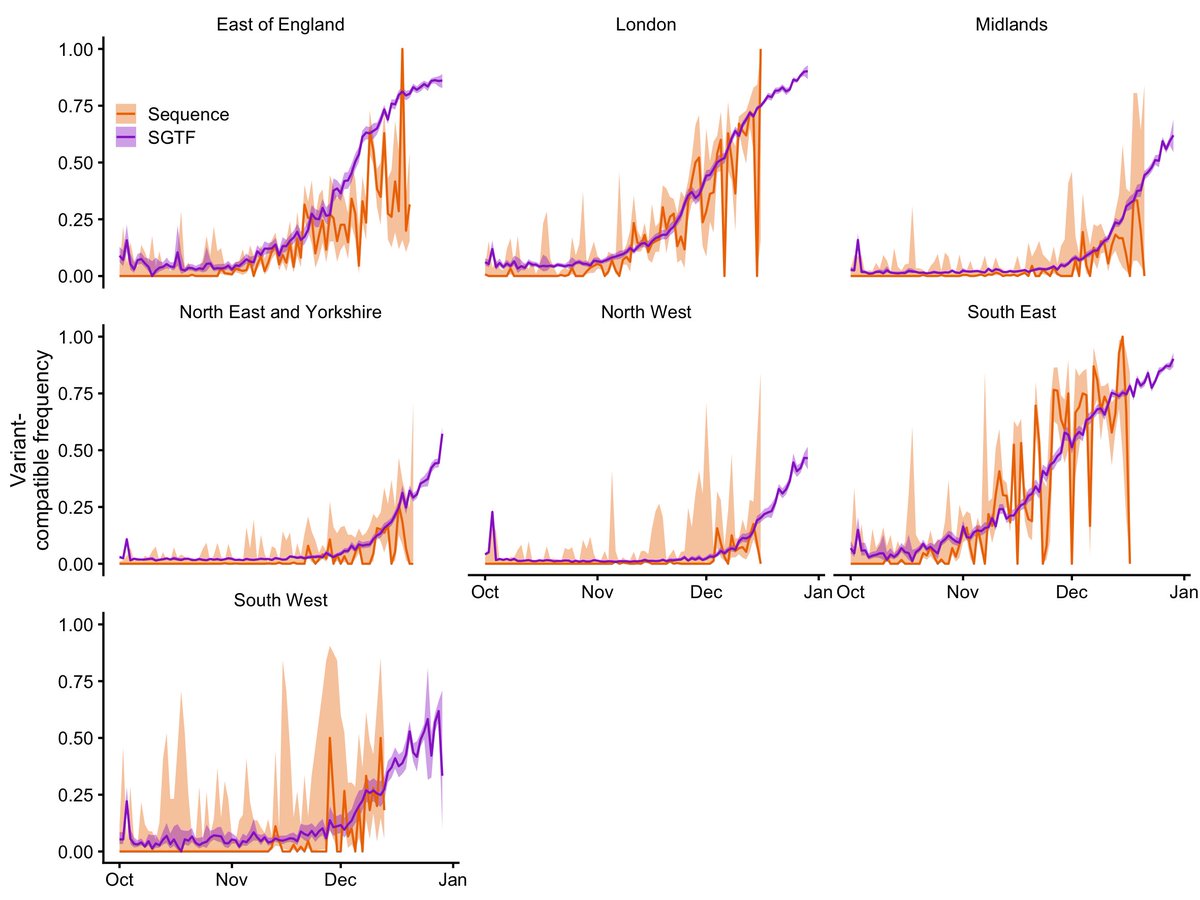
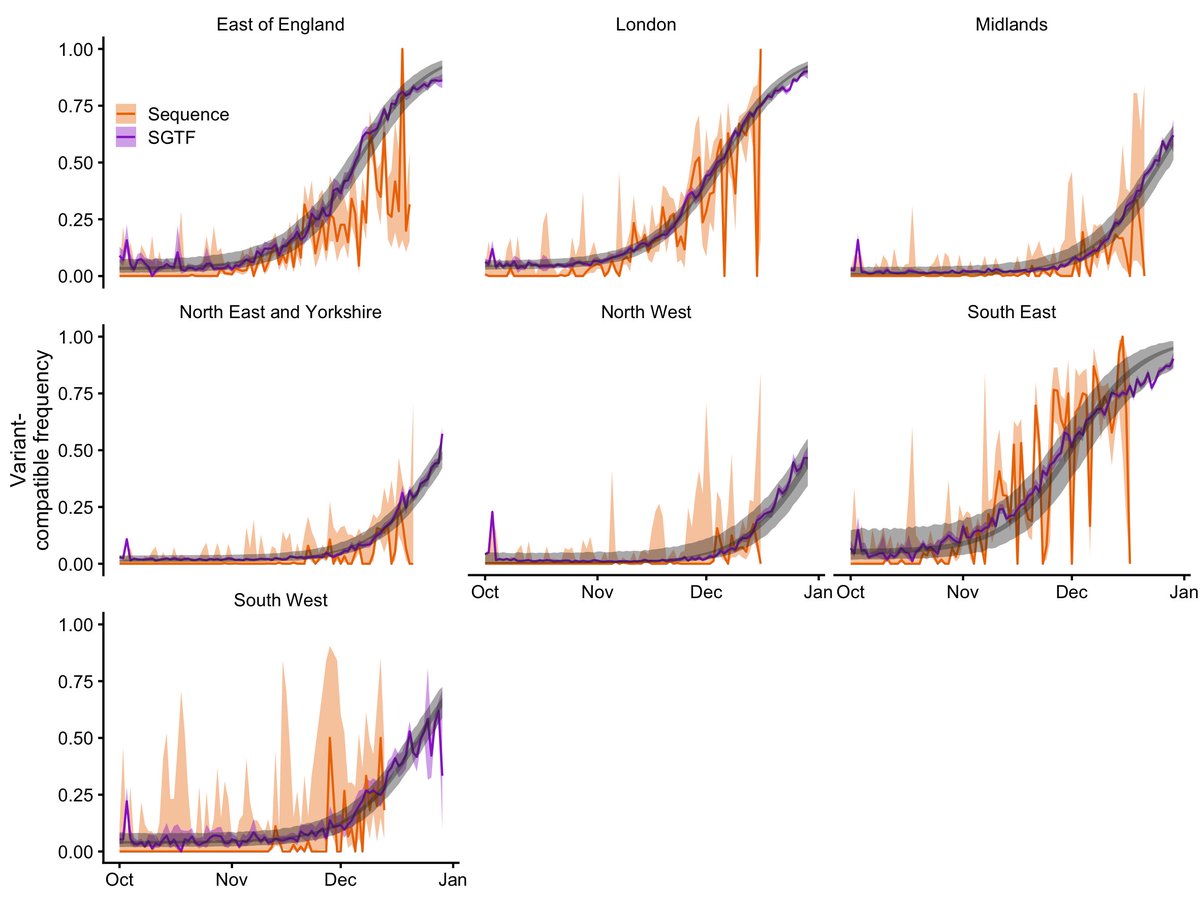
We now include new statistical estimates of B.1.1.7 growth, which accord with our earlier model-based estimates—and provide some really interesting plots. (thanks @Alex_Washburne, @inschool4life, @TWenseleers, @seabbs and @sbfnk!) UNDER PEER REVIEW (2/6)

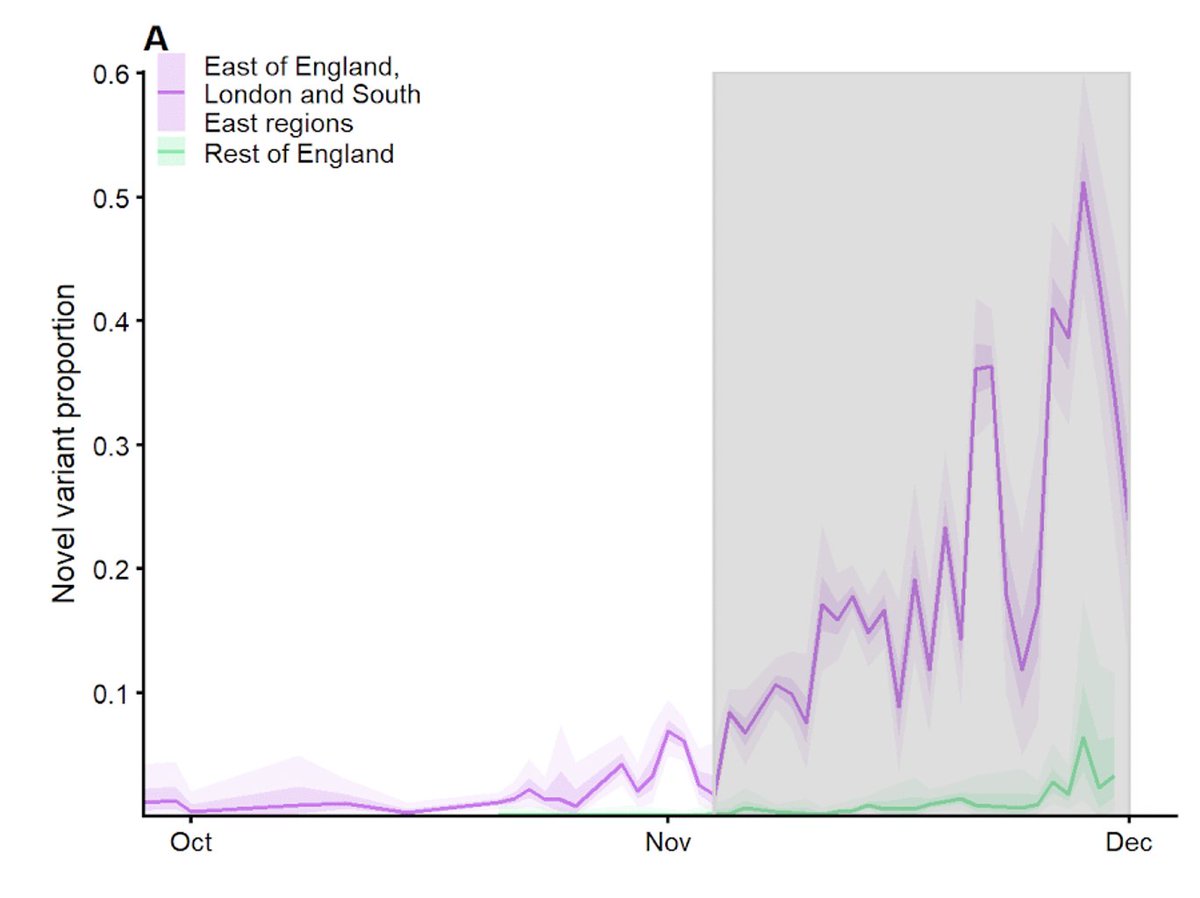
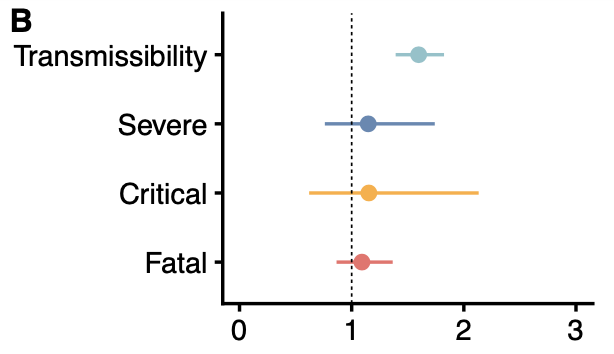
The estimates differ slightly, reflecting the different methods used. But they all identify a significant increase in transmissibility. Of particular note, we found similar growth rates in Denmark. See also, Belgium:
https://twitter.com/TWenseleers/status/1356994129125900296UNDER PEER REVIEW (3/6)

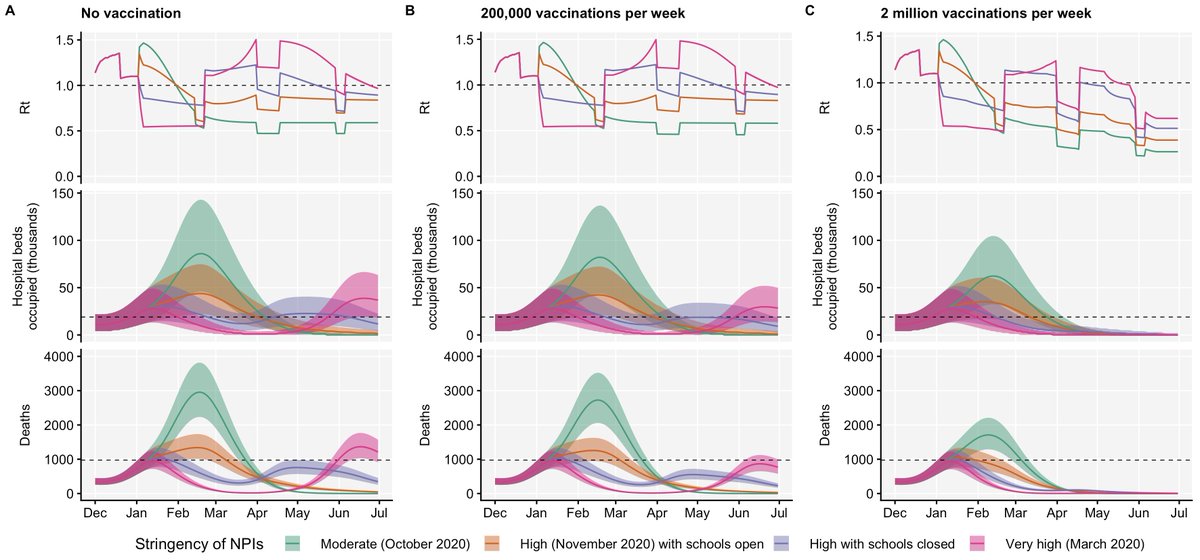
Our finding that vaccination is crucial to suppressing B.1.1.7 remains unchanged. UNDER PEER REVIEW (4/6)
Our median estimate of severity is moderately increased relative to preexisting variants. Very important to note, though, that this model is fit to early data where we might not expect to see a strong signal of severity. UNDER PEER REVIEW (5/6)
Thanks to all co-authors! We resubmitted this to the journal a few weeks ago. Looking forward to this hopefully being fully PEER REVIEWED very soon (6/6).
• • •
Missing some Tweet in this thread? You can try to
force a refresh