primary concerns re COVID are: fatalities, ICU &hospitalization, which vary by age group. Not easy finding data granular enough to examine interactions. Nor are such details discussed collectively (as they should) in Ontario science briefings. Here is (hard-won) Toronto summary. 
while COVID impact on ICUs has been a (if not the) primary focus of "Science Table" briefings, the number of fatalities is about 2.5 times higher than number of people who've gone to ICU. Mostly people over 80 who've died in community or in non-ICU hospital wards.
fatality rates of over 80s (and over 70s) in ICUs is very high: 70% (61%) respectively, while recovery rate of under 50s is very high (86%).
whereas the number of fatalities is concentrated in over80s, the largest cohorts in ICU are 60-69 and 70-79.
my takeaway from looking at this data in an overall way is that, to be blunt, ICUs are involved in only a very small percentage of COVID cases and need to be considered in a spectrum of options, rather than as the central policy issue.
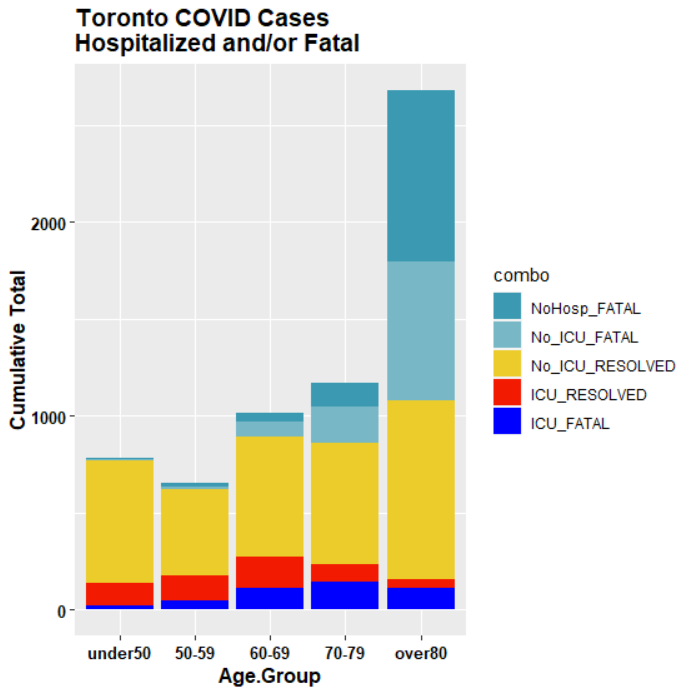
here's a better diagram of impacts by age group. Vast majority of cases, especially in younger ages recover without hospitalization. Left panel shows outcomes for all cases; right panel for cases in which hospitalization/fatality occur. ICU and fatality patterns are not the same.

2/ case loads among over-80s come disproportionately from LTCs. So vaccinations in LTCs will have an immediate impact on severe outcomes - whereas vaccinations of under-40 HCWs, deserving as they are, will have negligible impact on severe outcomes.
3/ however, ICU occupancy is concentrated more in 60-79 age group than in over-80s. This age group is less represented in LTCs. It is unfortunate that we don't have data on accommodation circumstances of 60-79s entering ICU.
4/ speaking as a 73-year old, I would prefer that society not lockdown on my behalf and that people of my generation take precautions to stay out of harm's way as much as possible and that vaccine priority be given to those that do not have that option.
5/ another age group graphic for Toronto, additionally disaggregating LTC (predominant form of "Outbreak"). Vaccinating the very small number of people in Toronto LTCs (~14K) by itself should immediately cut serious outcomes (ICU/Fatality) by ~50%.
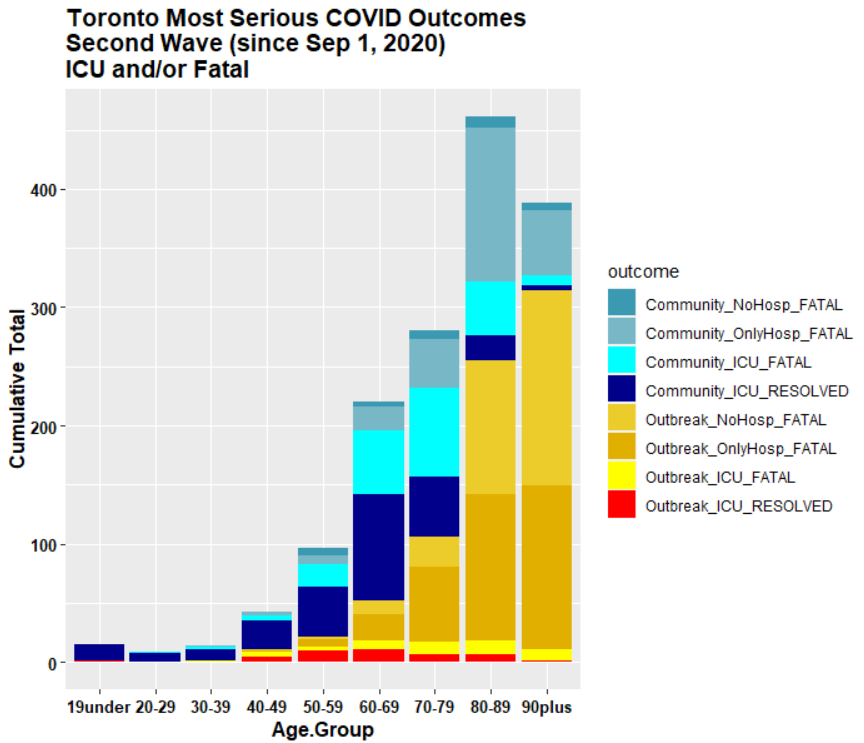
6/ that public health advisors and ethicists chose not to allocate very first 14K vaccines to this population defies all logic.
7/ But now that they've been vaccinated, issue is moot - other than some backbiting from public health scientists complaining that govt didnt vaccinate LTCs soon enough - even though these priorities had been set by public health advisors themselves. A bunch of mini-Faucis.
• • •
Missing some Tweet in this thread? You can try to
force a refresh