Unfortunately this @nytimes model uses unrealistic assumptions, like "80% of the population is ultimately fully vaccinated".
Even if *every* adult is vaccinated, that's still not 80% of the population. And we haven't even factored in vaccine hesitancy.
nytimes.com/interactive/20…
Even if *every* adult is vaccinated, that's still not 80% of the population. And we haven't even factored in vaccine hesitancy.
nytimes.com/interactive/20…
Rather than clearly highlighting this bold assumption in the article, it's buried at the bottom as a footnote.
At what point do unrealistic model assumptions become misleading? Does the science support immunity lasting indefinitely? Or 80% of Americans getting fully vaccinated?
At what point do unrealistic model assumptions become misleading? Does the science support immunity lasting indefinitely? Or 80% of Americans getting fully vaccinated?

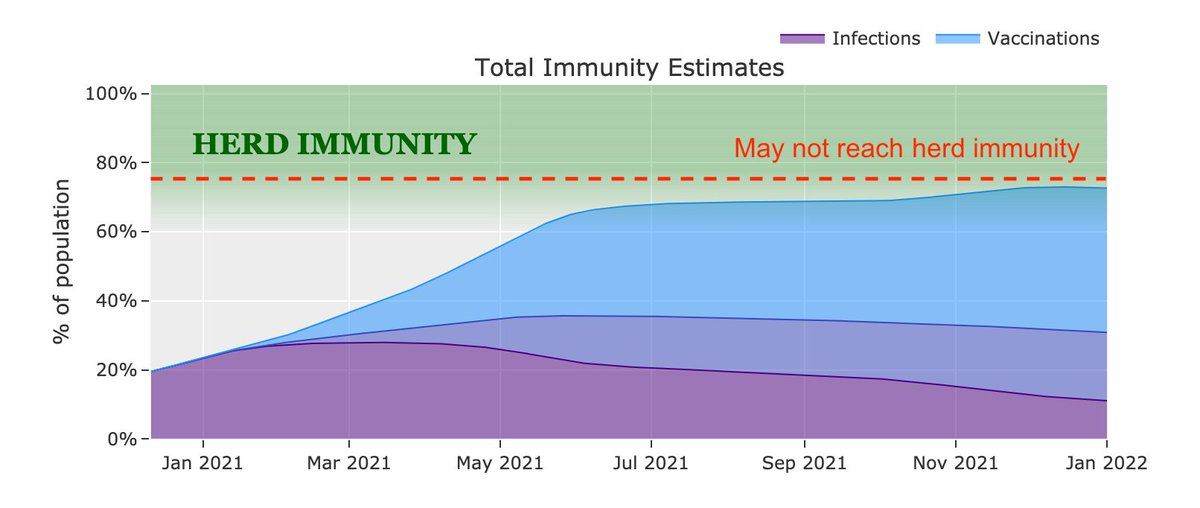
If the model used more realistic assumptions based on real-world data, they would probably conclude that we won't reach herd immunity. But that would likely break the premise of the model, so I can see why they chose not to explore this.
https://twitter.com/youyanggu/status/1359941463757516802
P.S.: Nice graph and title.


A follower pointed out this travesty as well.
It's 2021 and I can't believe we are still trying to push this narrative.
It's 2021 and I can't believe we are still trying to push this narrative.

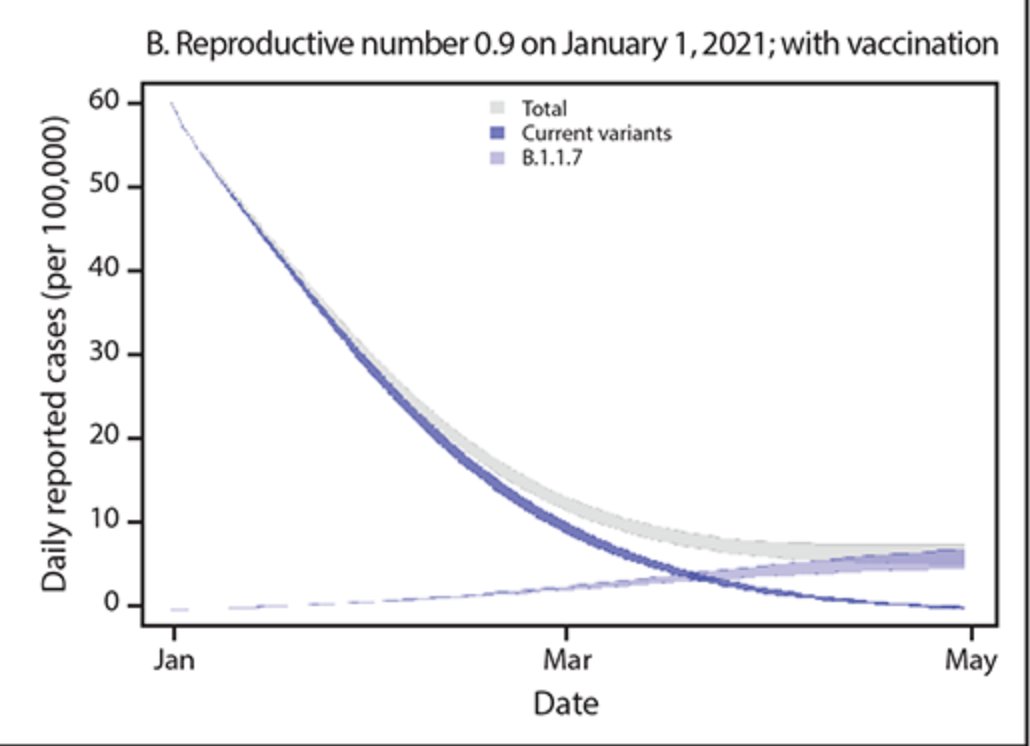
"Let's use an exponential function to model the variant".

But hey, it got 42k likes on Instagram...

• • •
Missing some Tweet in this thread? You can try to
force a refresh