The Richard Soppitt book chapter is interesting, there are some issues with it. I will probably do a full lists of pros/ cons with the piece in the next few days.
Need to check his version of the original 15 PDA DISCO questions by Wing & Gould.
Need to check his version of the original 15 PDA DISCO questions by Wing & Gould.
Unsure they align to what Gillberg et al (2015), or other information I have on the topic. For one, he seems to be conflating passive early history with speech delay questions, which were either in full DISCO/ removed.
The PDA literature contradicts itself over if there were 17/ 15 original PDA DISCO questions.
Interesting case study and comments about trauma.
Interesting case study and comments about trauma.
Interesting points on Wing & Gould's thoughts. Does not seem to mention how Wing & Gould commented prematurely on Newson's work in 2002, seem not to properly engage with Newson's work though.
I am unsure Soppitt himself has, mentions Newson's views on PDA lacking ToM deficits, does not mention her proposed Coding issues for it being in social identity/ pride shame/ instead.
His comments on Wing & Gould saying socially inappropriate behaviours are random & then negatively reinforced through attention sounds plausible; is inline with my comments on such behaviours as described by Harry Thompson.
Seems to ignore how Green et al (2018a) said PDA can be seen in non-autistic persons...
Seems to miss the contradiction in what he says about PDA, demand avoidance being automatic, but yet behaviours can be displayed when CYP with PDA faces prospect of doing something they do not want/ choose.
Mentions Kaushik et al (2015), so that gets some thumbs up.
Still arguing PDA is seen as an ASD, thumbs down.
Interesting diagram on what PDA might be comprised of.
Still arguing PDA is seen as an ASD, thumbs down.
Interesting diagram on what PDA might be comprised of.
Oh boy he argues for approaches that are mainly low arousal in nature.
Also argues for CYP with PDA to be sent to mainstream schools. So that part about PDA segregating autistic persons is still valid :(.
Also argues for CYP with PDA to be sent to mainstream schools. So that part about PDA segregating autistic persons is still valid :(.
Seems to think PDA is both developmental and pervasive, despite good case it is neither...
Mentions how PDA is supported by mainstream organisations, mentions NAS, does not mention their COIs...
He has read some of my work, which is referenced, at least one is.
He has read some of my work, which is referenced, at least one is.
Minor one, but references are not all in alphabetical order.
Refers to manipulative PDA behaviours, this is a thumbs up.
Mentions PDA's non-compliance.
Mentions PDA's non-compliance.
His comments around, PDA being more akin to ADHD, trauma and their low resilience levels are in line with my own thinking on the topic.
Mentions caregiver stress, thumbs up.
Mentions caregiver stress, thumbs up.
Professionals should not go looking for signs of abuse, but threshold's for trauma in autism are lower. Plausible.
Seems to use subgroup/ subtype interchangeably.
Seems to use subgroup/ subtype interchangeably.
Actually asks if other names for PDA should be used. Thumbs up.
He actually asks some interesting questions, discussion points in the end. Thumbs up.
Mentions most of Newson's cases would meet DSM-5 ASD criteria, misses how that would mean there are NON-autistic cases with PDA in her work.
Mentions most of Newson's cases would meet DSM-5 ASD criteria, misses how that would mean there are NON-autistic cases with PDA in her work.
This is a rather mixed chapter. There is much I like about it. Much I could take issue with.
I do need to further investigate some points, particularly on the PDA DISCO questions; why has he not used the revised DISCO questions (an obvious question)?
I do need to further investigate some points, particularly on the PDA DISCO questions; why has he not used the revised DISCO questions (an obvious question)?
Question 8) How do you explain the profile to a student with the presentation? Would they put it in a less pejorative terms?
Note the implied controversy around "PDA", and how it is a horrible name.
Note the implied controversy around "PDA", and how it is a horrible name.
An interesting chapter, with some interesting points.
Could have been better though in some areas.
Will comment more later, after doing some more research on certain points.
Could have been better though in some areas.
Will comment more later, after doing some more research on certain points.
To clarify a point about the original PDA DISCO questions. Some say there were 17. Gillberg et al (2015) used 15, & assessed for speech delay using questions from full DISCO.
Which is partly why I did this:
rationaldemandavoidance.com/2020/11/24/two…
Which is partly why I did this:
rationaldemandavoidance.com/2020/11/24/two…
The question raised, is why he is using those ones, instead of the revised and still unvalidated 11 PDA questions in O'Nions et al (2016).
For the record I would rather use the original PDA DISCO questions, as they do not assume PDA is a form of autism. They assess for all of Newson's profile (mainly). This means one can do comparison studies for PDA in predicted populations with them.
Most predicted PDA populations are based on Newson's descriptions, which means needing to use tools that conform to her descriptions; as the revised PDA DISCO questions have taken on "autism-like" features.
A reason being PDA probably presents differently in non-autistic populations. this is something I mention in my recent YouTube videos.
*slightly differently*
One thing that bothers with the chapter is not noticing/ reflecting on the contradictions present in what he is saying, e.g. non-autistic persons with PDA Newson's cohort. Or PDA not being an ASD If mainly ADHD & trauma.
Still trying to be positive about it.
Still trying to be positive about it.
A plus point, Soppitt viewing PDA social demand avoidance as manipulative, supports my point that the original PDA DISCO questions viewed PDA social demand avoidance as manipulative, not "apparently" or "strategic".
This point is supported by two tools partly derived from these original PDA DISCO questions view PDA social demand avoidance as manipulative, including the EDA-Q. I also a comment from a reviewer confirming that PDA DISCO questions wording was changed.
In the revised PDA DISCO questions (see 11 questions in O'Nions et al, 2016).
Another interesting point is how Soppitt interprets PDA as being mainly ADHD & trauma; which in my view is partly supported by some research results.
It is intriguing how he uses manipulative, instead of "strategic", which is often used by those who view PDA to PDA as an autism subtype/ subgroup/ profile (you know who you are).
It highlights the importance of ones bias in interpreting PDA.
It highlights the importance of ones bias in interpreting PDA.
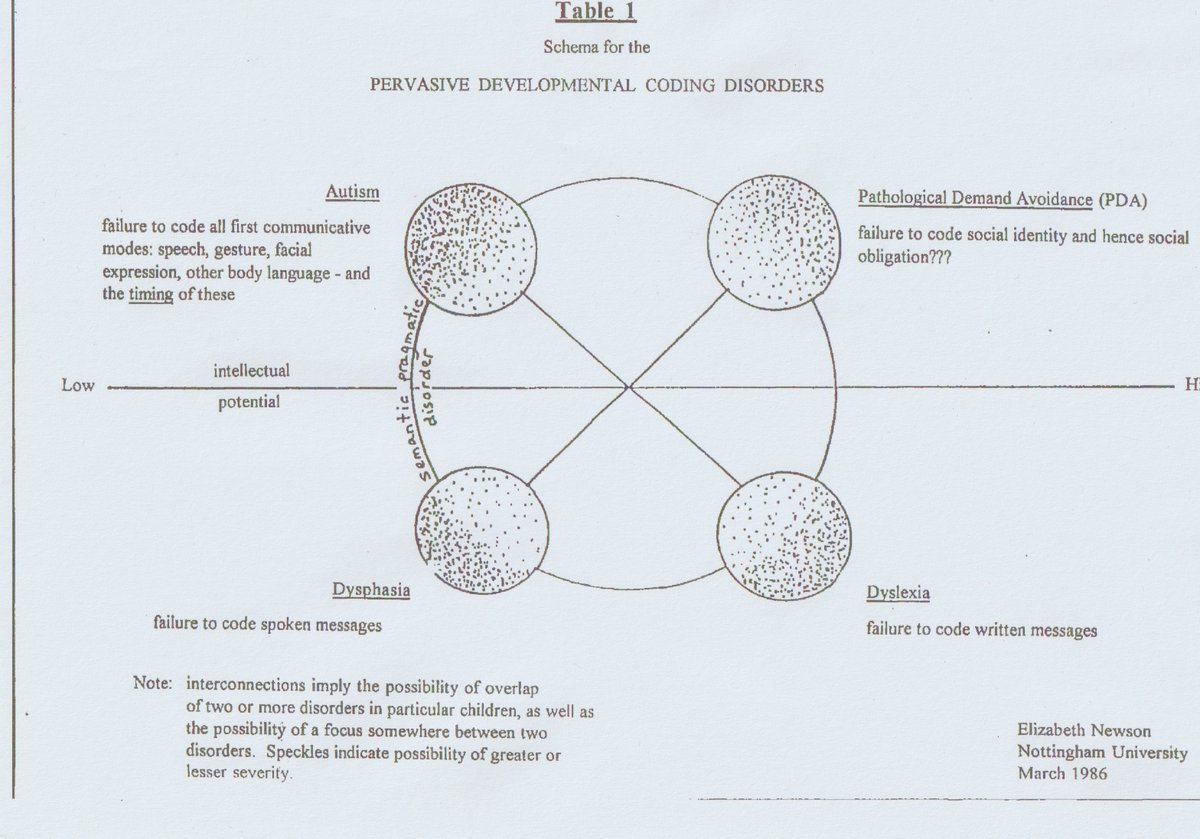
E.g. Newson requiring PDA to have coding issues in 1988, as she created her own Pervasive Developmental CODING Disorders group in 1986, which needs PDA to have coding issues. See Newson's notes on questioning what PDA's coding issues are. 
Reflecting on Soppitt is saying, about trauma in PDA, it raises the question on if he thinks people can transition INTO PDA after birth; which can happen under transactional accounts of PDA (a person can be distressed/ traumatised into PDA under such models).
Considering Wing repeatedly saying autistic persons can transition between subtypes, and later co-authoring these things can happen with Gould & Gillberg, that such issues are applicable to all proposed subtypes.
Suggests Wing (& probably Gould) have lower PDA dx thresholds than Help4Psychology. Supporting my point their PDA dx thresholds are at the extreme end what is available. This is something Soppitt misses when discussing Help4Psychology work.
For the record, if I update this diagram to include Wing's PDA dx threshold it would between Newson's & Eaton & Weaver as Newson diagnosed PDA in non-autistic person's.
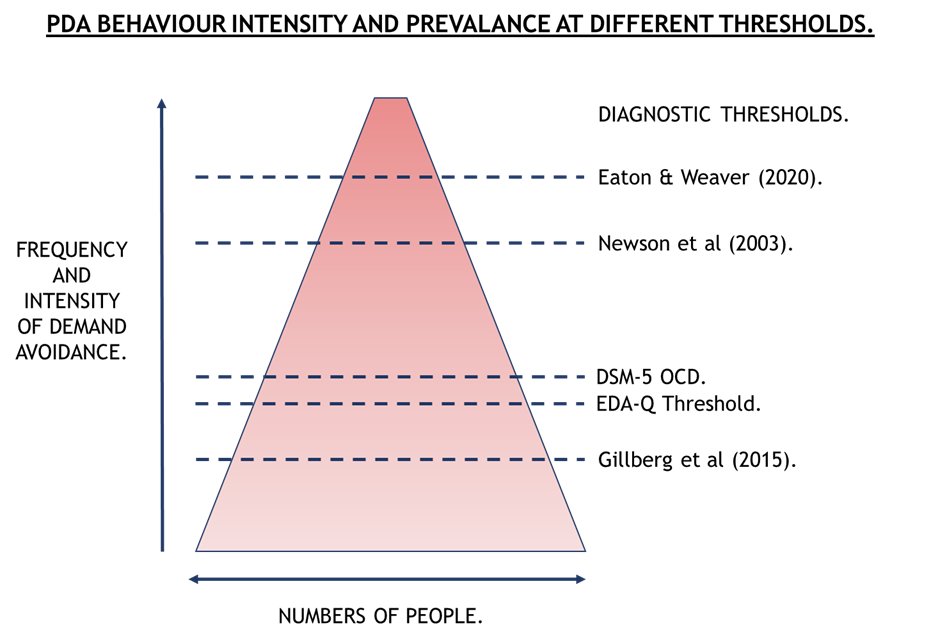
I doubt Wing (& Gould) ever knowingly diagnosed PDA in non-autistic persons as they view it as a form of autism. Newson held the opposite view, which Wing and Gould both seem to miss (they seem not to appreciate a lot of nuances of Newson's work).
Like Wing (& Gould), Newson herself said CYP can transition into PDA, she said this multiple times throughout her work.
I have updated the diagram to include Wing et al (2011), but in the draft blog post I will be explaining how it is probably representative of Wing's view's.

Although, I am considering if Soppitt's PDA definition is broader than Help4Psychology's PDA definition.
"There is typically no history of trauma, at least not in
the accepted sense of poor attachment/separation from a caregiver." (O'Nions & Eaton, 2020, p2).
the accepted sense of poor attachment/separation from a caregiver." (O'Nions & Eaton, 2020, p2).
"Likewise, children who have experienced developmental trauma in their early years can display behaviour that appears to be challenging as a result of a hyper-aroused sensory system." (O'Nions & Eaton, 2020, p2).
i.e. CYP with attachment issues can present PDA behaviours, just not O'Nions & Eaton's PDA definitions.
I would also add, from my understanding of attachment issues & its literature, PDA features are seen in this group.
researchgate.net/publication/33…
I would also add, from my understanding of attachment issues & its literature, PDA features are seen in this group.
researchgate.net/publication/33…
Soppitt argues that vulnerability to trauma drives PDA behaviour, this is inline with monotropism work for PDA in autistic persons.
Soppitt is probably correct to view much of PDA behaviour in case study as a panic response; that PDA is about stress management with limited coping strategies.
States its reasonable to view students with PDA as having a mixture of autism & trauma, p303.
40% of cases with PDA have trauma relating to having PDA, e.g. being restrained/ bullied for their behaviours. 25% trauma unrelated to PDA, e.g. death in the family
40% of cases with PDA have trauma relating to having PDA, e.g. being restrained/ bullied for their behaviours. 25% trauma unrelated to PDA, e.g. death in the family
p299.
"From my clinical experience of over twenty-five years in the field, ASD with features of PDA more often than not is correlated with ADHD and a trauma-type response, even if the external trigger is not obvious to parents or clinician." p 309.
"From my clinical experience of over twenty-five years in the field, ASD with features of PDA more often than not is correlated with ADHD and a trauma-type response, even if the external trigger is not obvious to parents or clinician." p 309.
Goes onto to discuss tolerance of demands in PDA, when resilience is low.
Again restates his points about ADHD and trauma responses are often inherent... p311.
Also says about confusion with attachment difficulties.
Only talking about PDA in autistic persons mind.
Also says about confusion with attachment difficulties.
Only talking about PDA in autistic persons mind.
I think one could view Soppitt's views as being more broader than Help4Psychology. They do not really go into as much detail as Soppitt though on this topic.
I have asked Judy Eaton, if Soppitt's PDA definitions are broader than Help4Psychology's.
I have asked Judy Eaton, if Soppitt's PDA definitions are broader than Help4Psychology's.
Bare in mind that PDA behaviours are seen in non-autistic persons, with similar mechanisms, relating to distress and high arousal.
"This is in line with other work with children with developmental disabilities, which describes distress, arousal and attempts to physically escape from demand contexts (Lucyshyn et al., 2004). (O'Nions & Neons, 2018).
That the EDA-Q detects PDA in non-autistic persons.
Highly informative to people, if a tool designed by several highly specialised autism experts to detect PDA in autistic persons, detects PDA in non-autistic persons, i.e. their view PDA is an ASD is wrong!
Highly informative to people, if a tool designed by several highly specialised autism experts to detect PDA in autistic persons, detects PDA in non-autistic persons, i.e. their view PDA is an ASD is wrong!
It does support the notion that PDA is a trauma/ distress response, it is primarily about stress management.
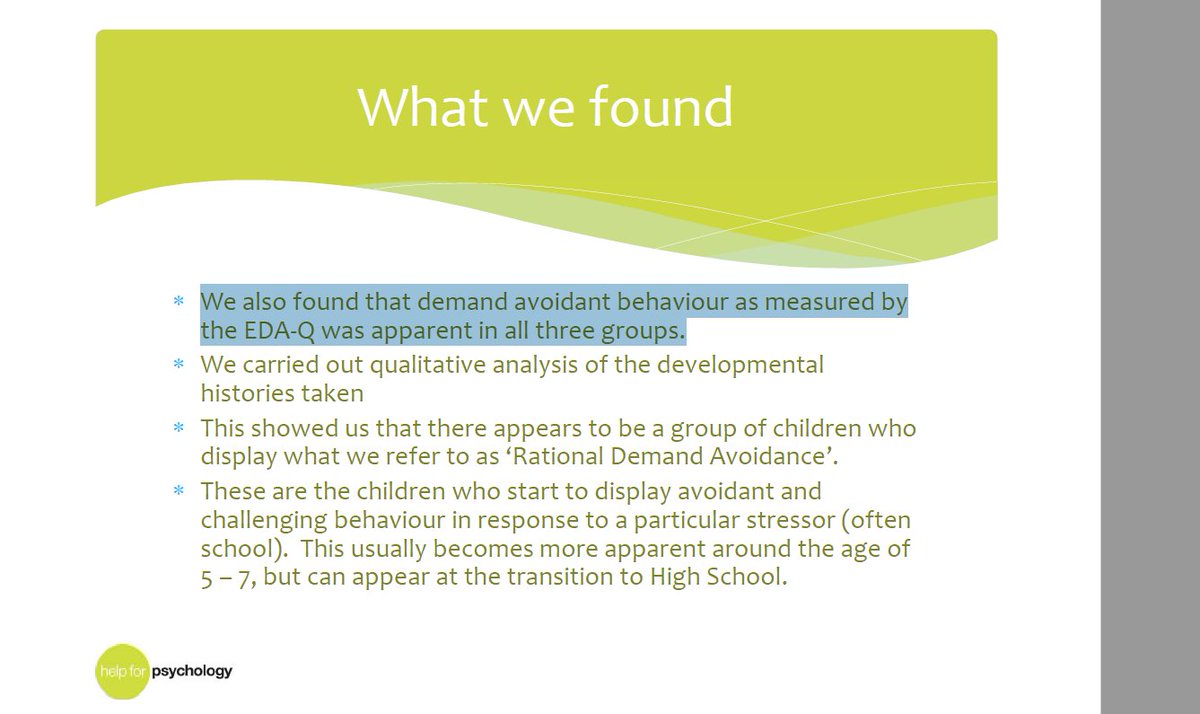
"We also found that demand avoidant behaviour as measured by the EDA-Q was apparent in all three groups" (Eaton, 2018).
Three groups in this case
Autism, no PDA.
Autism with PDA.
Other (trauma based group).
Three groups in this case
Autism, no PDA.
Autism with PDA.
Other (trauma based group).
This by Kaushik et al (2015).
"Eleven children (44%) scored above cut-off on the EDA-Q, 3 of which were diagnosed with ASD (43% of children with ASD)."
"Eleven children (44%) scored above cut-off on the EDA-Q, 3 of which were diagnosed with ASD (43% of children with ASD)."

Reilly et el (2014)
"significant symptoms of PDA, were assessed using the Extreme Demand Avoidance Questionnaire (EDA-Q)"
"Three, in addition, met criteria for ASD"
Note the one who does not meet autism dx threshold.
This is from the abstract.
"significant symptoms of PDA, were assessed using the Extreme Demand Avoidance Questionnaire (EDA-Q)"
"Three, in addition, met criteria for ASD"
Note the one who does not meet autism dx threshold.
This is from the abstract.
"The item list was sent to experienced clinicians (N = 10)... All ten were based in the United Kingdom, and worked in a range of specialisms and settings... The majority worked in highly specialist settings. (O'Nions et al, 2014, p759).
Bits that not included mentioning Gould & Christie were part of this 10, and other clinicians were known to Elizabeth Newson Centre. The breakdown of particular jobs of these clinicians.
The clinicians were consulted on candidate questions;
"additional items about early history and receptive verbal and nonverbal communication difficulties were included." (759).
"additional items about early history and receptive verbal and nonverbal communication difficulties were included." (759).
Considering the article viewed PDA as an ASD, & mainly attempts to differentiate PDA from autistic persons without PDA. Added to the types of questions added, i.e. included social communication issues.
Reasonable to assume many of these highly specialised clinical settings, are autism related.
• • •
Missing some Tweet in this thread? You can try to
force a refresh