I’ve spent a lot of time over the last 2 days going through the most recent paper thelancet.com/action/showPdf… from the Warwick modelling group that feeds into SAGE, and trying to work out why it predicts a large exit wave, when my model (mostly) doesn’t. My conclusions are: 1/12
1. Their model in fact doesn’t guarantee an exit wave: with fast vaccine rollout (4m per week) and high (85%) transmission blocking, and either high (85-95%) vaccine uptake or high (94%) protection vs. severe disease, there is no material exit wave - see the orange line 2/12 

2. Their choice of central assumptions is (imo) consistently on the pessimistic side. In fact, my central assumptions frequently correspond closely to their “optimistic” upside scenario. To avoid a very long thread I’ve built a table that compares their assumptions to mine 3/12

– so you can make your own mind up which is more realistic. The most surprising one for me was the vaccine rollout – their model central case has only 2.5m per week. And their assumptions for vaccine uptake and efficacy vs. severe disease still look a little light. 4/12
On the other hand, you could argue that I’m being a little too optimistic in my assumptions for R0, for starting immunity, and by including vaccination of teenagers in my base case – happy to concede on those points. 5/12
To explore this further I’ve built a ‘bridge’ from their model to mine, by feeding my model their assumptions (which produces pretty similar results to theirs, thankfully) and then changing the assumptions one-by-one to see what happens - see below, with commentary. 6/12


Apart from the fact that the Warwick model is persistently pessimistic in its choice of assumptions, what did we learn from that? Three more things, I think: 7/12
3. At the point of unlocking, we’re in a slightly weird place close to the herd-immunity threshold where small changes in assumptions can drive big changes in outcomes, and sometimes things don’t behave very intuitively. 8/12
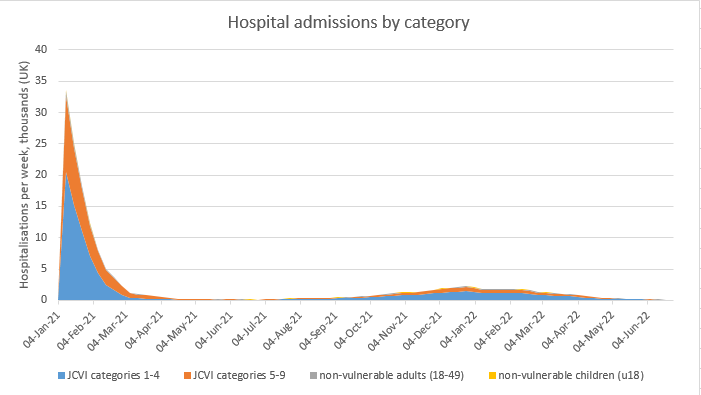
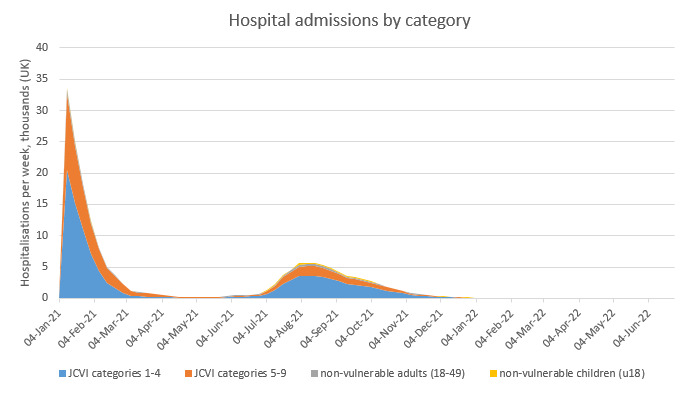
4. Overall, there is still a realistic possibility of an ‘exit wave’ with potentially up to 30k deaths, which depending on its speed, could come close to threatening NHS capacity – similar to our recent peak in December / January. 9/12
5. However, there is also a good chance that we avoid an exit wave entirely – if reality turns out slightly on the optimistic side of our assumptions for vaccine efficacy vs. infection, vs. severe disease, or for vaccine uptake – either way, it will be a close-run thing. 10/12
I am encouraged by the fact that Israel has opened up into a near-normal state (still with some masks and TTI, but other restrictions gone), and after what looks like a very small exit wave, cases are now falling fast (R~0.6). 11/12
https://twitter.com/segal_eran/status/1373876560030208006?s=20
My back-of-envelope calcs suggest we’ll be in a similar place on 21st June to where they are now, with around 70% of the population being protected by either vaccines or previous infection. If so, we should be able to open up in reasonable safety. 12 & end
@cjsnowdon you might be interested in this
• • •
Missing some Tweet in this thread? You can try to
force a refresh