What’s behind India’s second wave? A simple model can help us understand what’s going on.
There’s lots of variation between cities, so it’s best to look at a single city like Bangalore. Why did cases in Bangalore start to dip in Oct 2020? Why did they start to rise in Mar 2021?
There’s lots of variation between cities, so it’s best to look at a single city like Bangalore. Why did cases in Bangalore start to dip in Oct 2020? Why did they start to rise in Mar 2021?

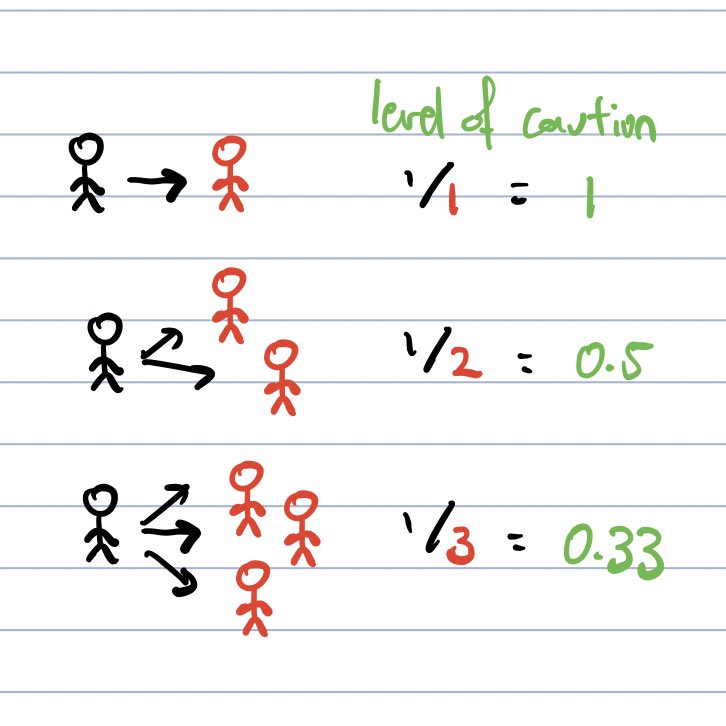
“R0” is the average number of new infections that would be caused by one infected individual, assuming nobody is immune. This depends both on behaviour and viral biology.
Let’s define the “level of caution” as the inverse of R0. Less cautious people cause more infections.
Let’s define the “level of caution” as the inverse of R0. Less cautious people cause more infections.
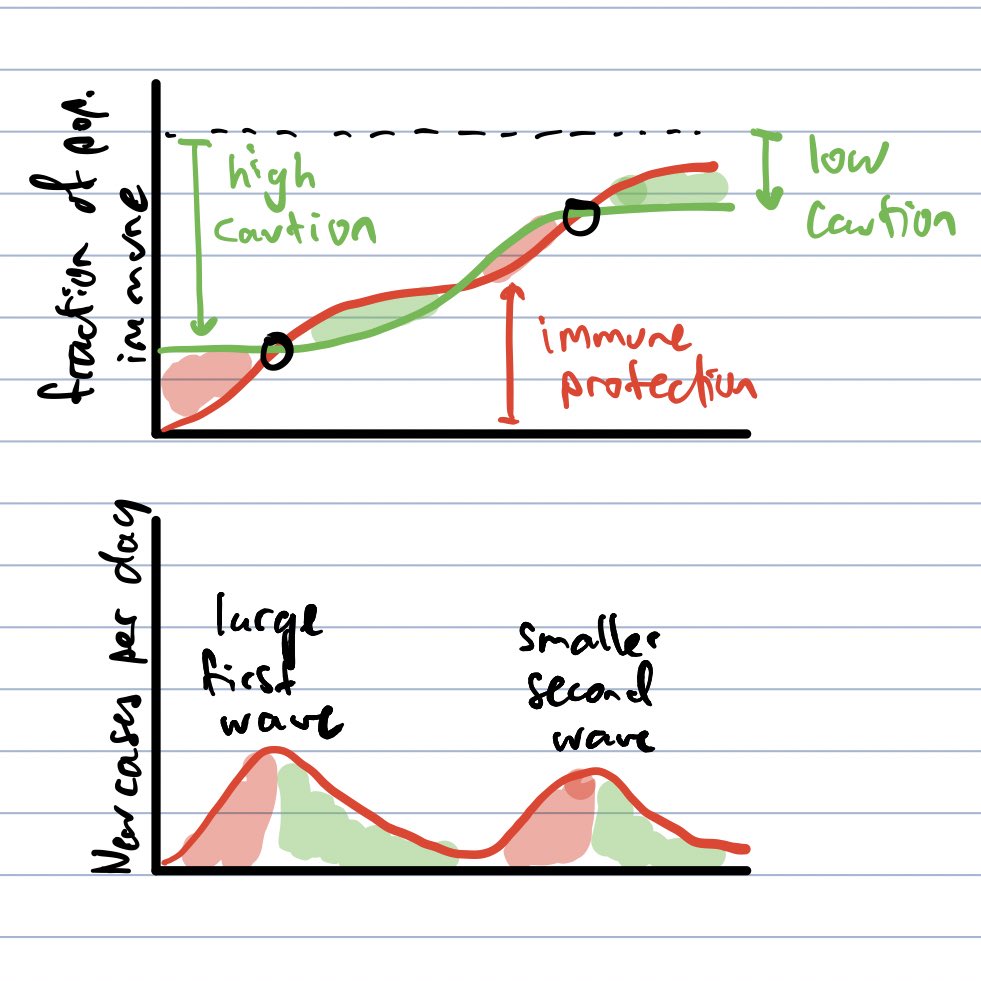
Let’s scale the y-axis from 0 to 1. In RED is the fraction of people who have recovered, and so are immune (measured from BOTTOM). In GREEN is the level of caution (measured from TOP).
When the red and green curves cross, new cases per day start to fall. This is “herd immunity”.
When the red and green curves cross, new cases per day start to fall. This is “herd immunity”.

What happens if we drop our guard? The level of caution drops, so the standing level of immunity is not enough to stop infections spreading.
More people get infected, until we hit a second herd immunity threshold. This kind of second wave is usually smaller than the first.
More people get infected, until we hit a second herd immunity threshold. This kind of second wave is usually smaller than the first.
After the first wave, broad immunity keeps new infections low even if people are less cautious, or if a more infectious strain arises.
But immunity fades. Someone who has recovered could be reinfected. The combination of less caution and less immunity drives a large second wave.
But immunity fades. Someone who has recovered could be reinfected. The combination of less caution and less immunity drives a large second wave.

Fading immunity is why “natural herd immunity” won’t end the pandemic.
But we can increase immune protection through widespread vaccination. (We may need annual vaccinations to deal with new strains or fading immunity.)
So stay cautious, and if you are eligible, get vaccinated!
But we can increase immune protection through widespread vaccination. (We may need annual vaccinations to deal with new strains or fading immunity.)
So stay cautious, and if you are eligible, get vaccinated!

• • •
Missing some Tweet in this thread? You can try to
force a refresh