1/ in our continued COVID field epidemiology series
"What's the question?"
April 2021 edition: "Are the vaccines effective against the variants?"
We have wet lab data, (limited) clinical trials reports, but what about field epi?
What epi design/surveillance would answer it?
"What's the question?"
April 2021 edition: "Are the vaccines effective against the variants?"
We have wet lab data, (limited) clinical trials reports, but what about field epi?
What epi design/surveillance would answer it?
https://twitter.com/Farzad_MD/status/1366225675481407488
2/ Why do I think it's "The Question" of this moment for field epi to try to answer?
I'm going to be joining @Bob_Wachter @cmyeaton @inthebubblepod tomorrow in our continuing "Safe or Not Safe" series, and Variant vs Vaccine will make all the difference
I'm going to be joining @Bob_Wachter @cmyeaton @inthebubblepod tomorrow in our continuing "Safe or Not Safe" series, and Variant vs Vaccine will make all the difference
https://twitter.com/Bob_Wachter/status/1380219686562881536?s=20
3/ I am 100% certain that everything I am saying here is much better understood by city/state epidemiologists @CSTEnews and @CDCgov experts.
But they are too busy to tweet, aren't free to talk openly, and may not control their own work/ resources.
And that's exactly the problem
But they are too busy to tweet, aren't free to talk openly, and may not control their own work/ resources.
And that's exactly the problem
4/ Here's some background most of you know.
People who are vaccinated have amazing protection against getting sick from COVID, and from transmitting it.
The best way to understand this is the probability distribution of vaccine efficacy
Great website:
wordpress.cels.anl.gov/covid-vaccine-…
People who are vaccinated have amazing protection against getting sick from COVID, and from transmitting it.
The best way to understand this is the probability distribution of vaccine efficacy
Great website:
wordpress.cels.anl.gov/covid-vaccine-…

5/ Vaccines also work well against the fast-spreading "UK Variant"
... except when it has the E484 mutation on top
nature.com/articles/s4158…
... except when it has the E484 mutation on top
nature.com/articles/s4158…

6/ The E484 mutation is what's maybe most worrisome about the "South Africa" (B.1.351) and "Brazil (P.1) variants.
We have limited data from clinical trials about vaccine efficacy vs these strains. Look at the confidence intervals in these estimates for Pfizer S Africa "finger"
We have limited data from clinical trials about vaccine efficacy vs these strains. Look at the confidence intervals in these estimates for Pfizer S Africa "finger"

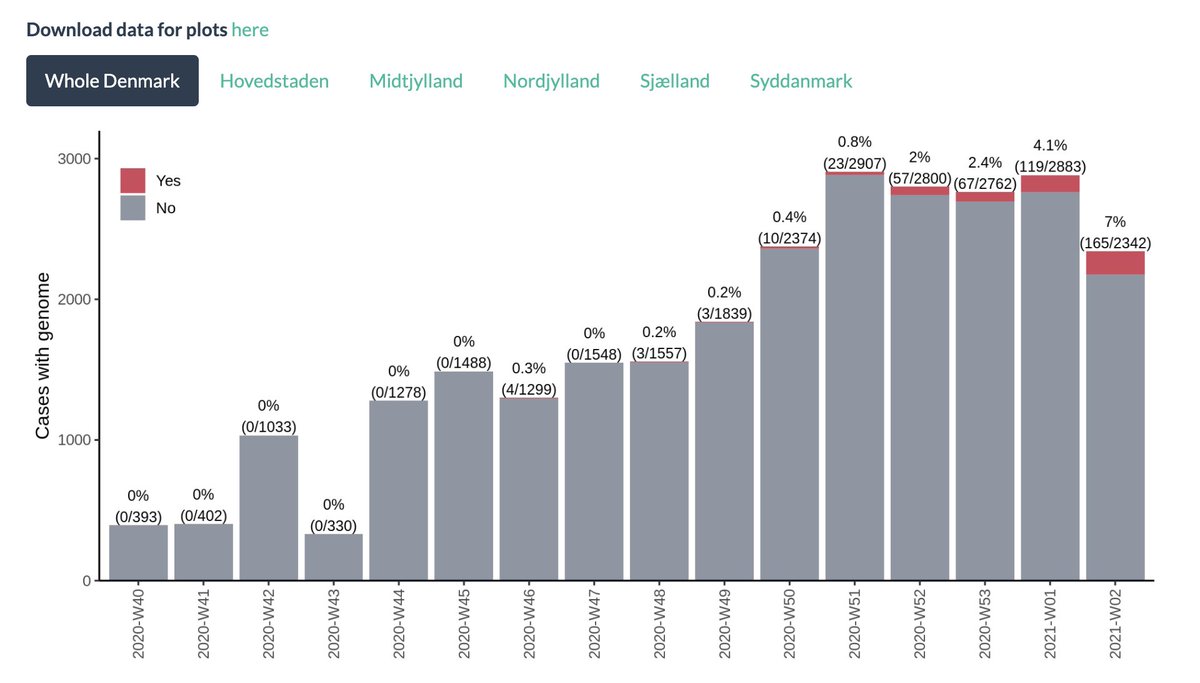
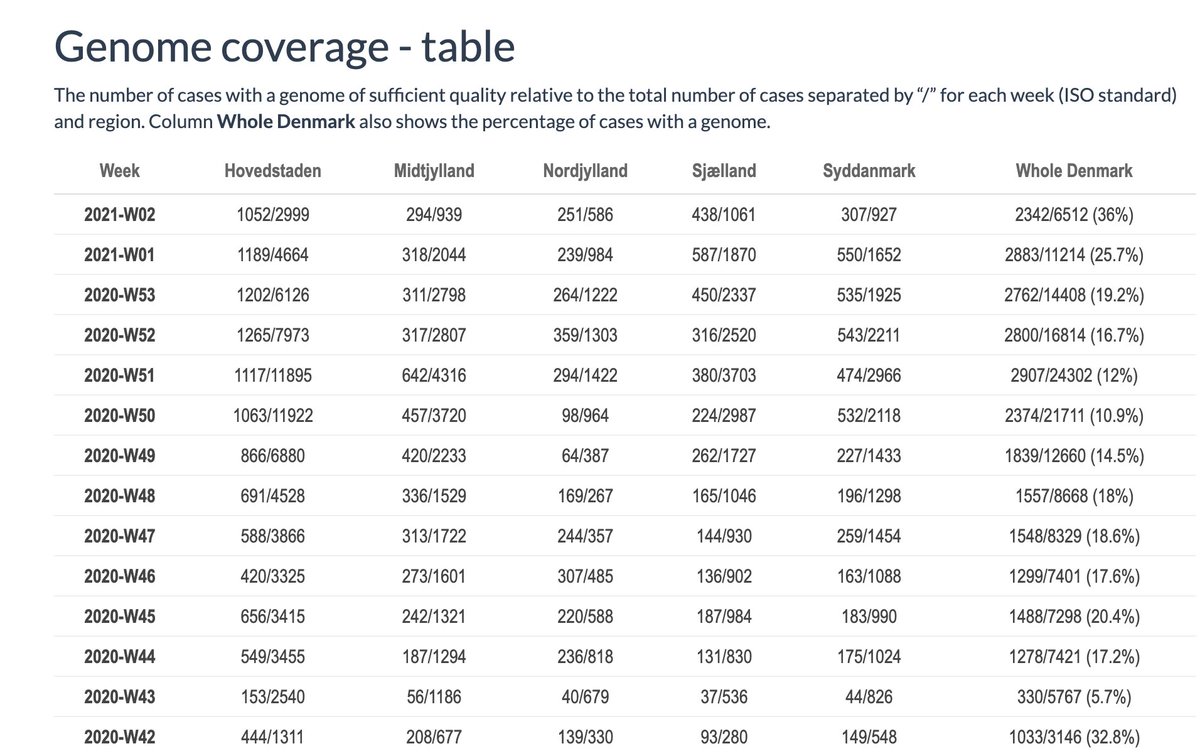
7/ How much are these strains circulating?
Thanks to this excellent dashboard from CDC (which should be better known) we can track it at a pretty granular level.
There's clearly community circulation in South Carolina (3% of sequences)
HT @dmaccannell
Thanks to this excellent dashboard from CDC (which should be better known) we can track it at a pretty granular level.
There's clearly community circulation in South Carolina (3% of sequences)
HT @dmaccannell
https://twitter.com/cyrusshahpar46/status/1380024885477474305?s=20

8/ And it appears to be spreading, albeit not fast.
So if I'm a vaccinated older person in South Carolina, can I ease off? Can I go ahead and hug my grandkids, as I suggested at the last @inthebubblepod?
Does it depend on which vaccine I got?
So if I'm a vaccinated older person in South Carolina, can I ease off? Can I go ahead and hug my grandkids, as I suggested at the last @inthebubblepod?
Does it depend on which vaccine I got?
https://twitter.com/inthebubblepod/status/1365380179523084291?s=20
9/ How can field epi answer this question?
You could sequence a representative sample of people who test positive, and look at likelihood of exposures (ie vaccine) in those with different strains of the virus.
**This is a perfect use of state/local contact tracing efforts**
You could sequence a representative sample of people who test positive, and look at likelihood of exposures (ie vaccine) in those with different strains of the virus.
**This is a perfect use of state/local contact tracing efforts**
10/ when I was an EIS officer in 1998 investigating a listeria outbreak I suggested that we use infected "cases" with non-outbreak strains as controls
(On the internet someone will tell me if I'm wrong)
This may have been a first for genetic field epi
ncbi.nlm.nih.gov/pmc/articles/P…
(On the internet someone will tell me if I'm wrong)
This may have been a first for genetic field epi
ncbi.nlm.nih.gov/pmc/articles/P…
11/ So we are doing tons of contact tracing investigations across the country.
In many places, we are so overwhelmed with cases that we can't think about design
Are we systematically collecting, validating and analyzing vaccination status in the course of those investigations?
In many places, we are so overwhelmed with cases that we can't think about design
Are we systematically collecting, validating and analyzing vaccination status in the course of those investigations?
12/ You know who does seem to be keeping their wits about them?
Israel.
Just published a case control study that does exactly this
medrxiv.org/content/10.110…
Israel.
Just published a case control study that does exactly this
medrxiv.org/content/10.110…

13/ In the unvaccinated infected population matched to the vaccinated carriers, only 0.7% of the sequenced variants were B.1.351. Among the fully vaccinated group (FE) it was 5.4%
That suggests a much lower rate of protection for B.1.351 than B 1.1.7
That suggests a much lower rate of protection for B.1.351 than B 1.1.7
https://twitter.com/RanBalicer/status/1380922662743126016?s=20

14/ There isn't a lot of B.1.351 circulating in Israel, but they were able to do this study nonetheless, on a population of 4.7M people (insured by @ClalitHealth)
why not us?
SC has more people than that. NYC is twice that (but contact tracing is done outside health dept).
why not us?
SC has more people than that. NYC is twice that (but contact tracing is done outside health dept).
15/ We have allocated a lot of money for state/local contact tracing efforts, but they are still overwhelmed
The lag time between symptom onset and initiation of contact tracing means we aren't getting much outbreak suppression for the effort.
The lag time between symptom onset and initiation of contact tracing means we aren't getting much outbreak suppression for the effort.
https://twitter.com/Farzad_MD/status/1297260001833230337?s=20
16/ I strongly believe that we should instead use these contact tracing efforts in a more thoughtful, DESIGN-ful way, so they can answer specific epi questions.
Children as vectors. Workplace transmissions. Super-spreader risks. Vaccinated carriers. Vaccine escape. & the next Q
Children as vectors. Workplace transmissions. Super-spreader risks. Vaccinated carriers. Vaccine escape. & the next Q
• • •
Missing some Tweet in this thread? You can try to
force a refresh