
During Friday's debate with @kprather88 and @DFisman, Dr. Conly raised a fairly common counter-point for why he thinks COVID is NOT Airborne: the relatively low Secondary Attack Rate (SAR) and Reproduction Rate (R0).
Let's unpack this flawed argument in a 🧵
1/
Let's unpack this flawed argument in a 🧵
1/
Dr. Conly states the SAR is 3 to 10%, with a household mean of 18%.
He then correctly points out that there is significant heterogeneity within the data, which means some people transmit to no contacts, while others transmit to everyone.
2/
He then correctly points out that there is significant heterogeneity within the data, which means some people transmit to no contacts, while others transmit to everyone.
2/
After admitting to the heterogeneity, he cautions we "have to be careful not to draw conclusions" from these superspreaders... eg. Chalet (73% SAR), Choir (53%), and Diamond Princess (58.9%). He suggests there were "extenuating circumstances", and seems to dismiss them. 🧐
3/
3/
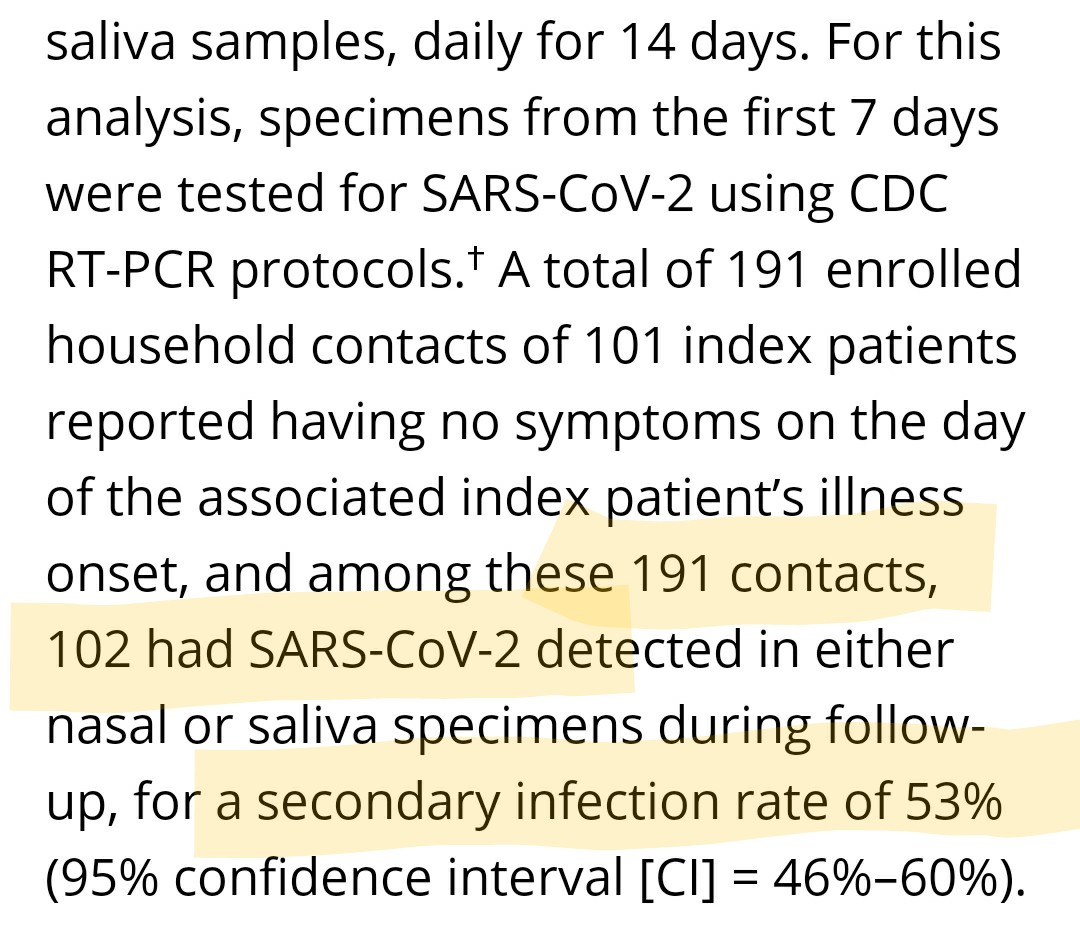
First note of caution... there are several recent studies that suggest a higher SAR than what Dr. Conly has referenced. Here's one from the CDC, which finds a SAR of 53%.
cdc.gov/mmwr/volumes/6…
4/
cdc.gov/mmwr/volumes/6…
4/
The early SAR studies often had testing limitations, where asymptomatic/presymptomatic cases weren't tested/followed up.
A recent paper looking at Dutch households (SAR of 35% to 51%), dives into this:
5/
academic.oup.com/cid/advance-ar…
A recent paper looking at Dutch households (SAR of 35% to 51%), dives into this:
5/
academic.oup.com/cid/advance-ar…

Dr. Conly also doesn't touch on the household SAR of the more transmissable variants, which anecdotely in Ontario, appears to be closer to 100%.
6/
https://twitter.com/drmwarner/status/1376342274301423619?s=19
6/
The other argument made by Dr. Conly, is that the R0 is "consistently in the range of droplet/contact viruses".
7/
7/
Is it though?
1) Estimates for R0 of measles range from 5 to 20+ (see thread)
2) Other estimates for R0 of SARS2 are as high as 11..
3) Why wasn't TB plotted? Its an Airborne virus and the R0 is ~3 🧐
wwwnc.cdc.gov/eid/article/26…
royalsocietypublishing.org/doi/10.1098/rs…
8/
1) Estimates for R0 of measles range from 5 to 20+ (see thread)
2) Other estimates for R0 of SARS2 are as high as 11..
3) Why wasn't TB plotted? Its an Airborne virus and the R0 is ~3 🧐
wwwnc.cdc.gov/eid/article/26…
royalsocietypublishing.org/doi/10.1098/rs…
https://twitter.com/CPita3/status/1378310134980612099?s=19
8/
Here's what the plot looks like when you include the variable R0 of measles, the variable R0 of SARS2 and the R0 of TB.
Not so clear cut now, is it? 🧐
9/
Not so clear cut now, is it? 🧐
9/

As an aside, R0 of an Airborne virus makes little sense to me. The number of people infected in a scenario, will be heavily dependent on ventilation. It would be better to have an R0 normalized by ACH, or some other measure of fresh air. Then you can compare apples to apples
10/
10/
So why the vast variability in R0 and SAR for SARS-CoV-2 across these studies?
This is indicative of the overdispersed nature of this virus, which @DFisman explains here:
11/
This is indicative of the overdispersed nature of this virus, which @DFisman explains here:
11/
Dr. Fisman explains this Overdispersion via 2 Epiphanies:
1) Variability in Aerosol production, depending on vocalizing activity and variability in Aerosol build-up depending on environmental conditions
12/
1) Variability in Aerosol production, depending on vocalizing activity and variability in Aerosol build-up depending on environmental conditions
12/
2) Variability in Viral Load from person to person and by day of infection
Put all of these together (variability in aerosol generation, ventilation and viral load), and it becomes obvious why this virus is so overdispersed.
13/
Put all of these together (variability in aerosol generation, ventilation and viral load), and it becomes obvious why this virus is so overdispersed.
13/
So the heterogeneity in the SAR/R0 is actually extremely important.
The overdispersion means the superspreader events are driving the Pandemic.
This is elaborated on further in this Nature article.
14/
nature.com/articles/d4158…
The overdispersion means the superspreader events are driving the Pandemic.
This is elaborated on further in this Nature article.
14/
nature.com/articles/d4158…
In the debate, Dr. Conly dismissed the high SAR in superspreader events due to "extenuating circumstances".
Those circumstances were likely:
1) Significant Aerosol generation
2) Poor ventilation and
3) High viral load
When combined, they create a perfect storm.
15/
Those circumstances were likely:
1) Significant Aerosol generation
2) Poor ventilation and
3) High viral load
When combined, they create a perfect storm.
15/
The only reasonable explanation for these superspreader events, which are driving the overdispersion, is Aerosol Transmission.
To suppress the Pandemic, we should target our interventions to prevent Aerosol Transmission, no matter how rare some experts think it is.
end/
To suppress the Pandemic, we should target our interventions to prevent Aerosol Transmission, no matter how rare some experts think it is.
end/

• • •
Missing some Tweet in this thread? You can try to
force a refresh





