
Des nouvelles de B.1.1.7, le « variant anglais » qui était censé provoquer un tsunami en raison de sa transmissibilité accrue, à partir des dernières données de Santé publique France 😂 

Même chose mais quand on fait la comparaison uniquement avec la souche historique plutôt qu’avec tous les variants non-B.1.1.7. En gros, la première méthode est sans doute un peu biaisée, tandis que celle-ci ne l’est pas mais l’erreur de mesure est plus grande.
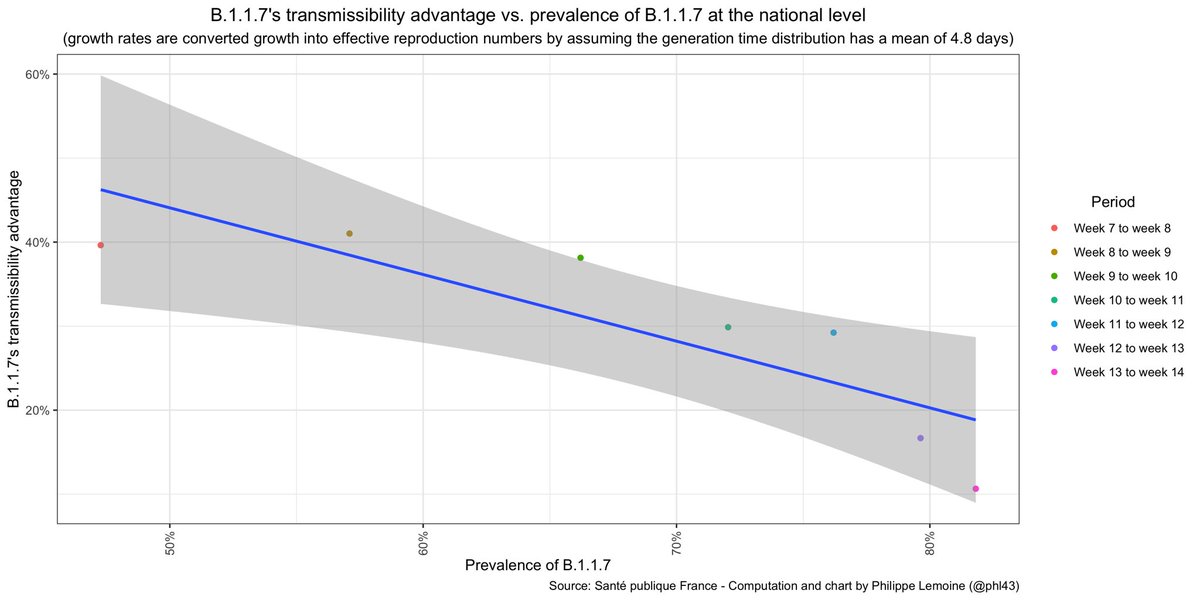
Je rappelle que les génies de l’Inserm et de l’Institut Pasteur continuent de faire l’hypothèse qu’il est 50% à 70% plus transmissible dans les modèles qu’ils utilisent pour faire les projections qu’ils présentent au gouvernement 👌
Mais ne vous méprenez pas, ceci n’est pas une critique des experts, pas du tout ! Je n’oserais jamais mettre en doute la compétence et l’intégrité de ces gens, qui ont sans doute une excellente raison de continuer à utiliser une estimation reposant sur les données de janvier.
Je dis ça parce que, pour un esprit qui n’est pas rompu aux subtilités de l’épidémiologie des maladies infectieuses, c’est vrai que ça peut donner l’impression que ces gens sont des guignols et qu’ils se foutent de notre gueule, mais rassurez vous c’est juste une impression 😌
• • •
Missing some Tweet in this thread? You can try to
force a refresh


