Not only did your study show no such thing, but it rests on demonstrably false assumptions, so it's really extraordinary that you continue to peddle those results. Here is a thread in which I explain why this study is worthless and should never have been used to guide policy 🧵
https://twitter.com/vcolizza/status/1382941421968183298
First, the model used in that study assumes that B.1.1.7, the UK variant, is 59% more transmissible than the historical lineage. This estimate is based from Gaymard et al. (2021), which obtained it by fitting a simple exponential growth model to only 2 data points from January.
As I explained at length in this post, even if we just use those 2 data points from January, this estimate is highly sensitive to the assumptions we make about the distribution of the generation time and there is a lot of uncertainty about that. cspicenter.org/blog/waronscie…
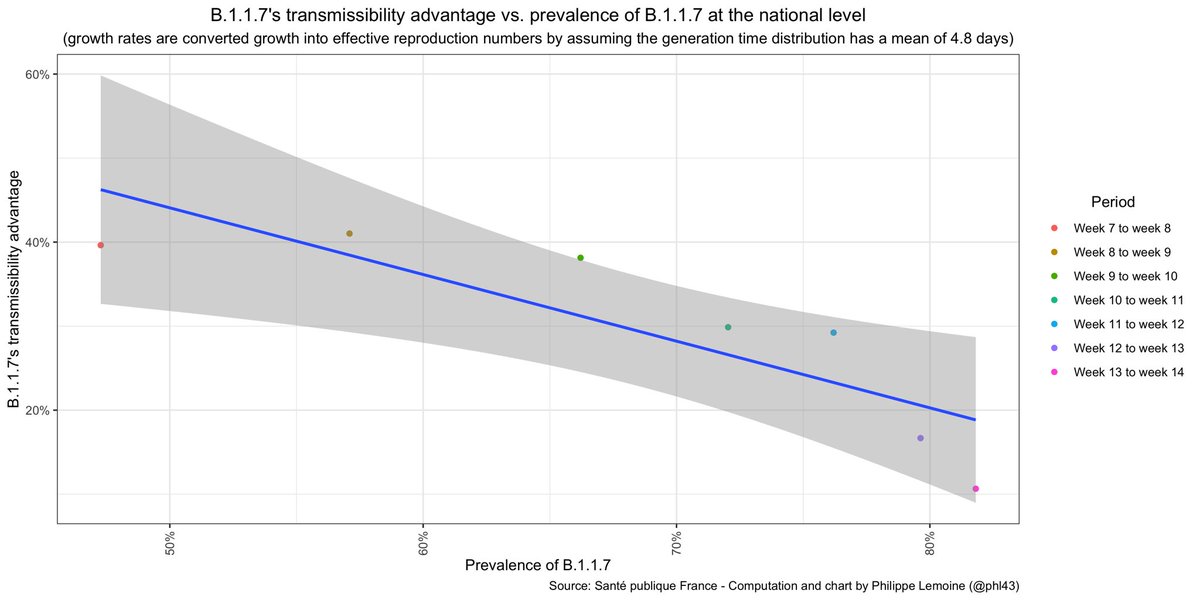
But more importantly, the data show *very* clearly that B.1.1.7's transmissibility advantage has totally collapsed in France since January, so the estimate of 59% that you use in that paper is completely outdated and therefore your results are totally worthless. 

You claim that your study "showed" that advancing the curfew from 8pm to 6pm in January is what prevented the explosion, but this result is meaningless because it was already baked into the model, something you know very well but totally ignore when you talk to the public.
Basically, you told your model that a 59% more transmissible variant had been introduced in the population and fed it hospitalization data until the end of February, which showed no explosion.
Since there was no explosion despite the rise in prevalence of a supposedly 59% more transmissible variant, the model had to ascribe that to *something*, but it's set up in such a way that there is nothing else it could ascribe it to beside the curfew and the school holidays.
So obviously it ascribed the lack of explosion to the curfew and the school holidays, but what is that supposed to show? There was literally nothing else it could have ascribed it to, so this result is totally uninteresting!
In particular, the model couldn't have ascribed the lack of explosion to the actual reason, namely that B.1.1.7 doesn't have a constant transmissibility advantage of 59%, because again you just *assumed* that it did, even though you had data showing that's not true 🙃
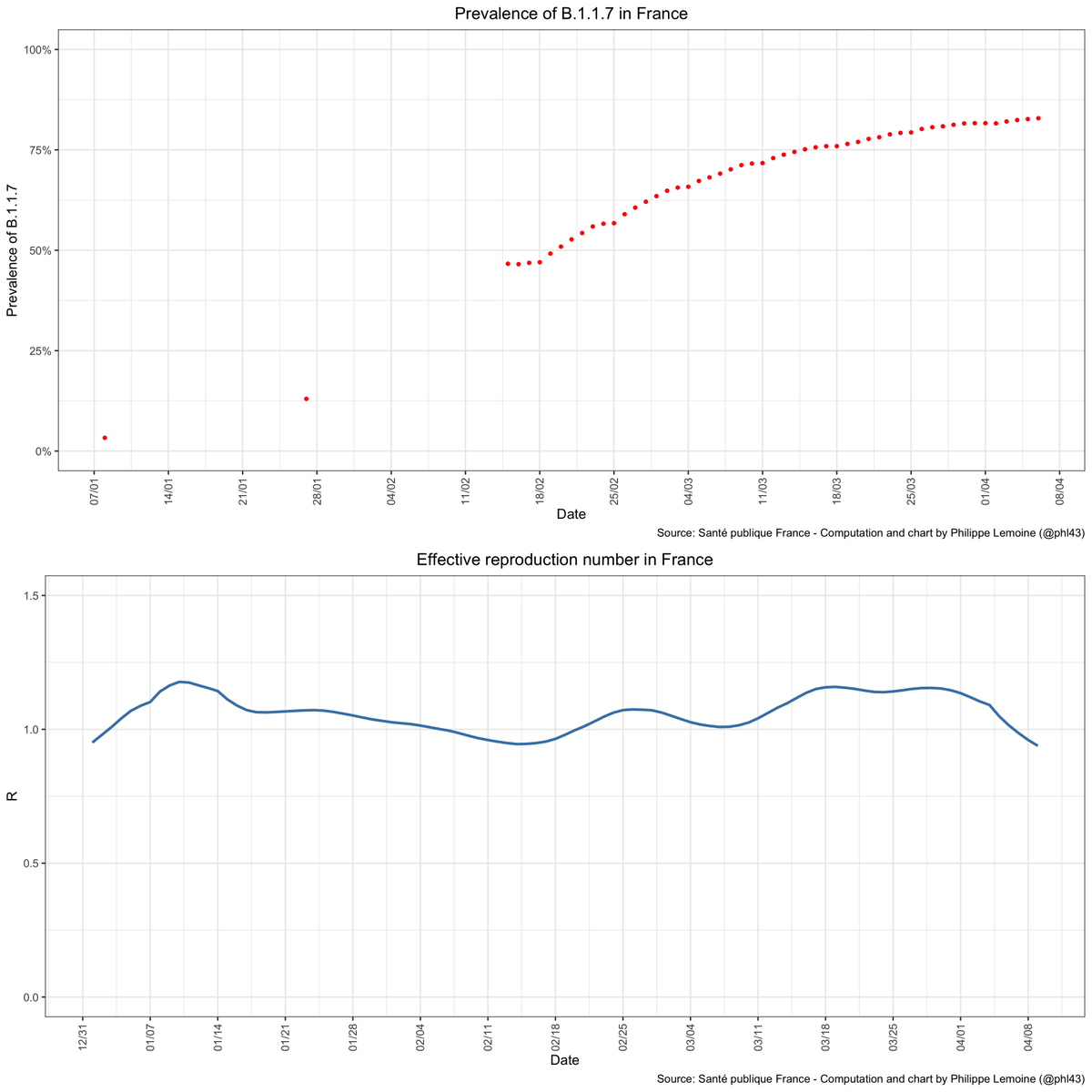
If B.1.1.7 really had a constant transmissibility advantage of 59%, R would have been *much* higher by the end of March and there would have been several hundreds of thousands of cases every day by then, which obviously didn't happen.
So pretending that what happened in March somehow validates your results is profoundly dishonest, because if your model were accurate, both R and incidence would have been *far* higher. Of course, you know that, but you also know that most people have no idea how this works...
If your code were available, we could say more about exactly how wrong your model was, but as usual you didn't publish it and you ignored me when I emailed you to ask if you could send it to me (we only have the code of a similar model you used in another paper), so we can't 🤷♂️
People should systematically publish their code, there is *no* excuse for not doing so, but it's even worse when you're paid on the public dime and keep your code hidden, as you have done since the beginning of the pandemic even though your work is used to guide policy.
Back to your study, it's really incredibly that, even though it rests on assumptions that are now *obviously* false, you totally ignore new data and continue to peddle its conclusions instead of admitting that your model was flawed and going back to the drawing board.
In addition to the fact that your model assumes that B.1.1.7 has a constant transmissibility advantage of 59%, something that again we *know* to be false, it ignores many factors such as voluntary behavior changes in response to changes in epidemic conditions.
The whole exercice has no practical relevance whatsoever and should never be used to guide policy, yet that's exactly what you do when you use those meaningless results to recommend tightening restrictions. You are a total fraud who knowingly misrepresent the import of your work.
• • •
Missing some Tweet in this thread? You can try to
force a refresh