
So I was flicking through these slides of Christie's in 2016
dp.dk/decentrale-enh…
There are some comments towards the end which I think are insightful, not necessarily for good reasons.
dp.dk/decentrale-enh…
There are some comments towards the end which I think are insightful, not necessarily for good reasons.




I will probably be critiquing these comments of Christie's over the next of couple of days, not necessarily in order.
This seems fair to me:
"Significantly improve awareness and understanding of PDA in adults"
This seems fair to me:
"Significantly improve awareness and understanding of PDA in adults"
"Cogent accounts and descriptions from clinicians, teachers and parents"
PDA resonates with those people. I do not how see how he can say this there is no agreed consensus over what PDA is. Viewing PDA to be ASD directly contradicts Newson views on the topic
PDA resonates with those people. I do not how see how he can say this there is no agreed consensus over what PDA is. Viewing PDA to be ASD directly contradicts Newson views on the topic

"Emerging insights from those with PDA"
On surface is reasonable. Question over how much of what they are saying is from internalising main PDA discourse. Still need to validate lived experience of vulnerable people who display PDA features.
On surface is reasonable. Question over how much of what they are saying is from internalising main PDA discourse. Still need to validate lived experience of vulnerable people who display PDA features.
Also issue of what about non-autistic persons with PDA lived experience accounts?
Presumably as Christie views PDA to be a rare autism subtype, he would say they do not exist.
Presumably as Christie views PDA to be a rare autism subtype, he would say they do not exist.
"Growing awareness, recognition and interest from practionersand researchers"
Yes, not necessarily for good or ethical reasons, looking at Grahame et al (2020) rationale. Again, not always to because people agree with Christie's views and approach to PDA.
Yes, not necessarily for good or ethical reasons, looking at Grahame et al (2020) rationale. Again, not always to because people agree with Christie's views and approach to PDA.
Which considering reluctance of Christie and others to accept divergent opinions on PDA, is a bit of an issue.
"Wide acceptance of the construct of PDA within the UK autism community"
At the time in 2016, and I would argue today it not true. PDA is not diagnosed universally across the UK and for good reasons to! Again not accurate by Christie.
At the time in 2016, and I would argue today it not true. PDA is not diagnosed universally across the UK and for good reasons to! Again not accurate by Christie.
"An active, considered and growing parent organisation"
This would be @PDASociety, not sure why he is stating this as something good that has been achieved. It just shows that a significant amount of caregivers have brought into Christie's outlook on PDA.
This would be @PDASociety, not sure why he is stating this as something good that has been achieved. It just shows that a significant amount of caregivers have brought into Christie's outlook on PDA.
"refine our understanding of the ESSENTIAL criteria and the core difficulty with social identity"
Essential is italicised in slides.
Essential is italicised in slides.
This is a hugely problematic one, also informative.
So it does support wider literature that PDA traits were deliberately reduced by removing developmental traits.
Now this would also mean that one could remove Surface Sociability trait...
So it does support wider literature that PDA traits were deliberately reduced by removing developmental traits.
Now this would also mean that one could remove Surface Sociability trait...
Which I am pretty sure Christie would disagree with as he views PDA to be an ASD. Fundamental issue of "core difficulty with social identity", which I am still unsure of how they that is being reliably assessed.
Garralda pointed out that features in this trait do not often reliably measure core deficit of lack of social identity in PDA. Features like, "sense of right and wrong" (whose perspective), being afraid of and for their child. Are both subjective.
"Some of the features outlined (for example sense of identity, price and shame) would be specially difficult to identify reliably."
adc.bmj.com/content/88/7/5…
adc.bmj.com/content/88/7/5…
I would also point out that many of other features of trait with "deficits in pride/ shame/ identity" are RRBIs, like panic attacks.
I am unconvinced there ARE such deficits in PDA (see the slide). So a rather big assumption here by Christie.
I am unconvinced there ARE such deficits in PDA (see the slide). So a rather big assumption here by Christie.
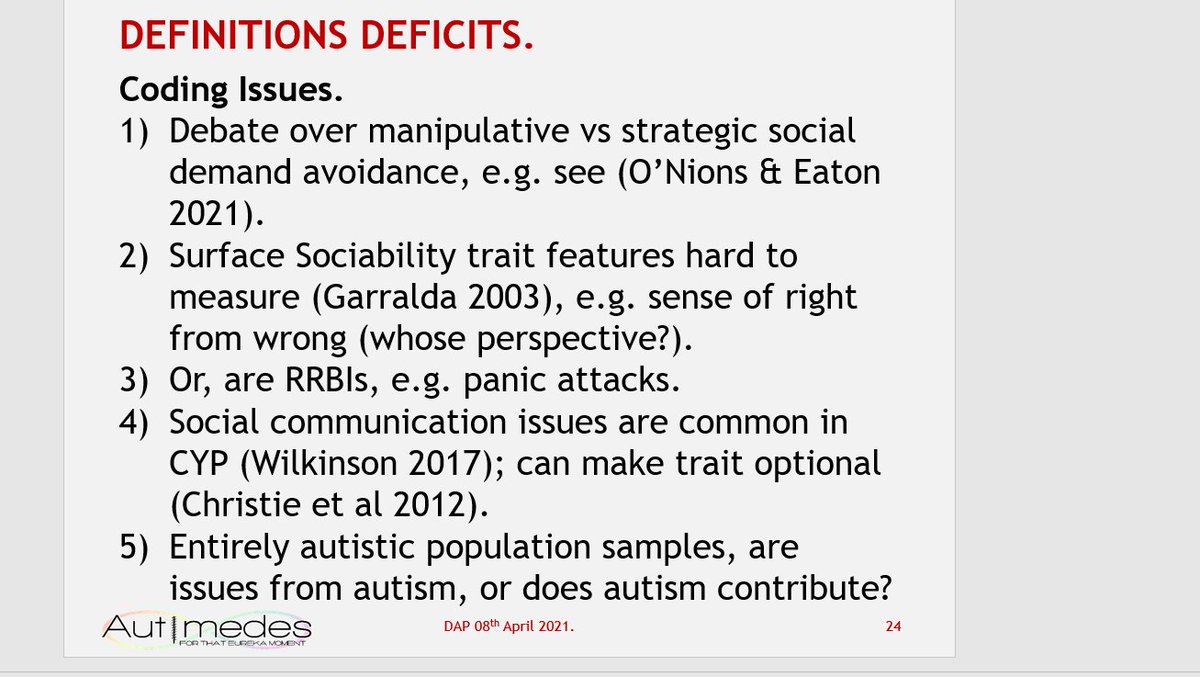
Debate over manipulative vs strategic social demand avoidance, e.g. see (O’Nions & Eaton 2021).
Surface Sociability trait features hard to measure (Garralda 2003), e.g. sense of right from wrong (whose perspective?).
Surface Sociability trait features hard to measure (Garralda 2003), e.g. sense of right from wrong (whose perspective?).
Or, are RRBIs, e.g. panic attacks.
Social communication issues are common in CYP (Wilkinson 2017); can make trait optional (Christie et al 2012).
Entirely autistic population samples, are issues from autism, or does autism contribute?
Social communication issues are common in CYP (Wilkinson 2017); can make trait optional (Christie et al 2012).
Entirely autistic population samples, are issues from autism, or does autism contribute?
I will come back to this later.
Has Christie critically reflected on this point "core difficulty with social identity"? Viewing PDA's social communication issues as due to that & not Theory of Mind makes it problematic viewing PDA as an ASD. How can supposed deficits cause panic attacks?
*these supposed deficits in pride/ shame/ social identity cause panic attacks?*
These kind of logic issues underscore my point about lack of cogent clinical descriptions on PDA.
These kind of logic issues underscore my point about lack of cogent clinical descriptions on PDA.
Another example, from Christie's 2007 article. He mentions that many of Newson's cohort of PDA would receive a diagnosis of Asperger's/ atypical autism (a residual category for those not meeting threshold for Asperger's/ autistic disorder).

Logically, if not all of Newson's cohort meet DSM4/ ICD10 threshold for autism subtypes, then there are some non-autistic persons in Newson's cohort. Then by definition PDA cannot be autism.
Likewise, if PDA is not based on the triad of impairment, which we know Newson never based PDA on the triad of impairment (I know its now a dyad). Again, logically PDA is not an ASD. Just because PDA is a similar to autism, does not make it an ASD.
This is what I mean, the clinical descriptions around PDA are NOT cogent as argued by Christie.
It raises more questions of the Christie's coauthor researchers like @HappeLab & O'Nions. Are they critically engaging with PDA & telling Christie of such issues?
It raises more questions of the Christie's coauthor researchers like @HappeLab & O'Nions. Are they critically engaging with PDA & telling Christie of such issues?

"Better understand areas of ‘overlap’ and ‘co-morbidity’ or co-existence"
This seems reasonable. We need greater consensus over what PDA and how to assess it first.
This seems reasonable. We need greater consensus over what PDA and how to assess it first.
"Reach broader consensus on use criteria and classification in diagnosis"
That sounds reasonable to me, others would disagree with it. Both sides have merit.
That sounds reasonable to me, others would disagree with it. Both sides have merit.
I would point out need stop assuming PDA is an ASD first in order to do that, as it allow for scientific -method based research and rights and wishes of non-autistic persons with PDA are equally respected.
"Develop research tools for use as screening and diagnostic guidelines"
Considering as there are currently no fully validated screening and research tools for PDA. Also a criticism of PDA is has no validated tools. It does seem reasonable.
Considering as there are currently no fully validated screening and research tools for PDA. Also a criticism of PDA is has no validated tools. It does seem reasonable.
"…future versions of diagnostic manuals"
Are a generation away...
Best place to start is work to standards of current diagnostic manuals, so their definitions & criteria. Which would mean broadening PDA criteria to lower thresholds.
Are a generation away...
Best place to start is work to standards of current diagnostic manuals, so their definitions & criteria. Which would mean broadening PDA criteria to lower thresholds.
There is also a point being made about arbitrarily shielding some autistic persons from ABA/ PBS (if one views PDA an ASD), considering their lack of relative effectiveness and apparent issues with causing trauma.
The DSM5 does not require PDA to be Pervasive or Developmental in nature. Likewise, if one focuses on "essential" traits relating to demand avoidance & wording of avoidance of ordinary demands trait.

The rationale for broadening PDA is a few factors, one is to match opinion PDA is seen in non-autistic persons & limited supporting evidence for this. To ensure people at lower diagnostic thresholds receive appropriate support.
That various diagnostic arguments for using PDA in autism, most/ all of them seem applicable to lower diagnostic thresholds of PDA.

Bottom comment here is. We do not know how much of it is: Christie seemingly not critically reflecting on PDA. And/ or his co-author's are critically reflecting on PDA & not informing him how it is problematic viewing PDA as an ASD?
https://twitter.com/Richard_Autism/status/1384104129593675784
Or how much Christie's researcher co-authors are not critically reflecting on PDA?
We do know that at in their early PDA scholarship @HappeLab & O'Nions both were pointing out it is problematic fitting PDA into autism.
Here
journals.sagepub.com/doi/10.1177/13…
&
pdaresource.com/files/An%20exa…
Here
journals.sagepub.com/doi/10.1177/13…
&
pdaresource.com/files/An%20exa…



Although looking at the comment that PDA represents features from other conditions, I would suggest it is valid. Not really an i ssue though (in my view) considering most disorders each overlap each other & are social constructs.
I would argue that generally PDA still lacks robust evidence, that is a tangent.
The reason why I am mentioning co-author researchers is that, one clinician who views PDA as an ASD, argues I am overly harsh in my critique as they are not researchers, they should not be held to same standards.
Not that accept that as an excuse. Clinicians have to research as part of their formal training. Also need to stay up to date with literature, so they should be able to recognise what is good practice from good quality research.
Although, I suppose one could argue that with much autism research being poor quality, autism specialist clinicians are not necessarily exposed to what "good practice" looks like.
The poor quality of much autism research, is partly why I am pushing for better quality PDA research. We really should be aiming for highest standards, but at least striving for good quality research & practice; better than much of PDA research.
Disclosing COIs, and not assuming PDA is an ASD would be start.
It is an issue if you are trying to make PDA something it might be comprised of, like autism. If PDA is not caused by autism, it cannot be autism. If PDA is comprised of features more than autism, it cannot autism. A + B + C ≠ A.
https://twitter.com/Richard_Autism/status/1384410637162491905

I have updated it to reflect how not all of Newson's cohort are autistic.

@threadreaderapp Please could you unroll?
• • •
Missing some Tweet in this thread? You can try to
force a refresh






