
We've refined a little more our Old Fake estimate as function of Ct values.
Madrid dataset we use included 3 Ct frames, <20, 20-30 & >30.
Our equation changes slightly:
%Old positivity=(Ct-28)/3
It brings a good approximate to calculated Old Detection:

Madrid dataset we use included 3 Ct frames, <20, 20-30 & >30.
Our equation changes slightly:
%Old positivity=(Ct-28)/3
It brings a good approximate to calculated Old Detection:
https://twitter.com/plaforscience/status/1383105140895444995?s=19
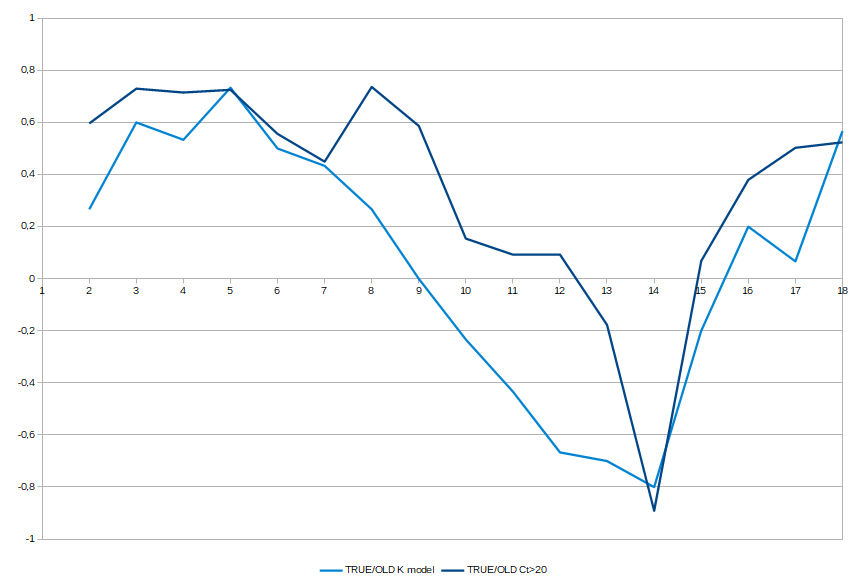
Method used for this refinement was considering all the Ct>20 as true positive and considering Average Ct for >20.
We observe the calculated Old Positivity fits with this average Ct, and we used to estimate the relation.
We observe the calculated Old Positivity fits with this average Ct, and we used to estimate the relation.

Our equation also models that every point the Ct Average grows, the Old Positivity increases ~30%, so around Ct~31 and over your detecting almost only Old Fake Positives.
Both cut limit at ~28 and no true detection at ~31 are coherent with the studies on virus viability in culture depending on Ct values.
We see the decline crosses the 50% precisely ~28 and then falls quickly until disappear at ~34.
Not bad for statistics with blurry data.
We see the decline crosses the 50% precisely ~28 and then falls quickly until disappear at ~34.
Not bad for statistics with blurry data.

• • •
Missing some Tweet in this thread? You can try to
force a refresh


















